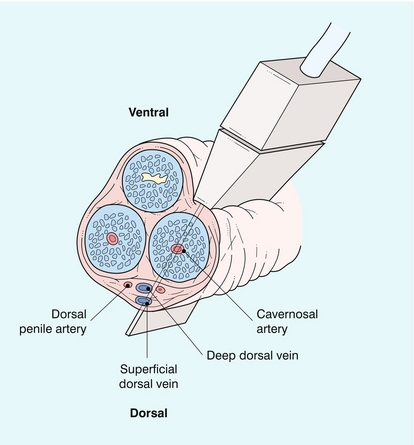
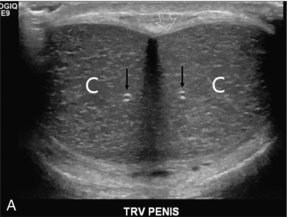
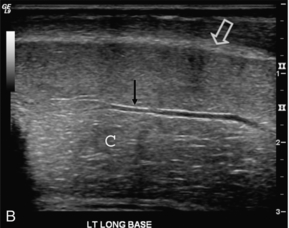
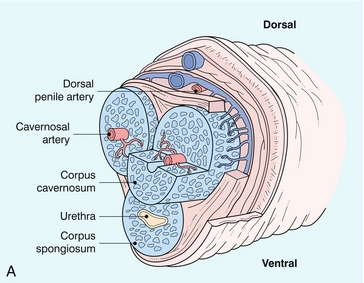
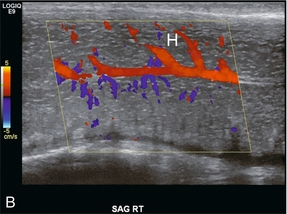
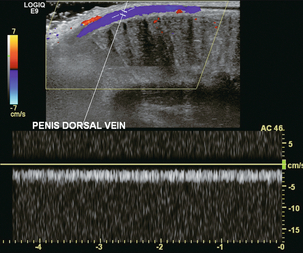
Chapter 12 The evaluation of erectile dysfunction (ED) has been the dominant application for penile Doppler, especially in the older population since the prevalence and severity of the disease increases with advancing age.1 While impotence may be the result of psychogenic, neurogenic or hormonal factors, vascular disease is the most common cause of ED.2 With the introduction of phosphodiesterase inhibitors [specifically Sildenafil citrate (Viagra©), Verdenafil HCl (Levitra©), and Tadalafil (Cialis©)], the frequency of Doppler studies for ED has significantly decreased.3 Most centres now prescribe a trial of the phosphodiesterase inhibitors as the initial diagnostic/therapeutic test of ED, with only non-responders being sent on for imaging. The penis contains three longitudinal, cylindrical erectile bodies. Two corpora cavernosa are located in the dorsal two-thirds of the penile shaft, and a single corpora spongiosum is located in the ventral one-third of the shaft. The corpora cavernosa are enclosed by the tunica albuginea, a tough, non-distensible fascial layer. The septum that divides the corpora cavernosa contains fenestrations that create multiple connecting anastomotic channels between the sinusoidal spaces, allowing for free communication across the midline. The dorsal arteries, veins and nerves are situated centrally along the penile dorsum, superficial to the tunica albuginea and deep to Buck’s fascia. The urethra is contained within the corpus spongiosium.4 On ultrasound, the corpora cavernosa are of uniform hypoechoic echotexture. The tunica can be seen as an echogenic envelope around the corpora. The echogenic walls of the cavernosal arteries can be seen centrally within the corpora. The corpus spongiosum is of higher echogenicity (Fig. 12-1). FIGURE 12-1 (A) Transverse and (B) longitudinal ultrasound images of a normal penis. The corpora cavernosa (C) have uniform echogenicity throughout. The echogenic tunica (open arrow) and echogenic walls of the cavernosal artery (arrows) are easily identified. The internal pudendal artery and its branches are the primary source of arterial supply to the penis. The first three branches are the superficial perineal artery, the bulbar artery and a small urethral artery. The perineal artery is a large and constant branch that, in 80% of cases, has an internal and external branch. The bulbar artery, which supplies the proximal penile shaft, is usually easily identified during angiography because it is associated with a bulbar parenchymal blush in the early arterial phase. The urethral artery, which is of small diameter, arises anterior to the bulbar artery. After these branches, the internal pudendal artery continues as the common penile artery. It then divides into left and right penile arteries, which enter the base of the penis and branch into a dorsal artery and a cavernosal artery. The dorsal artery extends along the dorsal aspect of the penile shaft towards the glans and terminates at the level of the arterial corona of the glans; it supplies blood primarily to the skin, subcutaneous tissues and glans. Collateral vessels from the dorsal artery often communicate with the cavernosal artery. The cavernosal, or deep penile artery, enters the tunica albuginea proximally and extends the length of the corpus cavernosum. The cavernosal arteries and their helicine branches are the primary source of blood flow to the erectile tissue of the penis. Just as the cavernosal artery supplies blood to the corpus cavernosum, the spongiosal artery supplies the corpus spongiosum4 (Fig. 12-2). FIGURE 12-2 Normal anatomy. (A) The cavernosal arteries are centrally located in each corpus cavernosus. The urethra courses through the corpus spongiosum. The dorsal penile artery supplies the glands and does not play a direct role in erectile function. (B) Colour Doppler reveals flow in the cavernosal artery and its helicine branches (H). Venous drainage of the penile erectile tissue (i.e. the sinusoidal spaces) primarily occurs through emissary (efferent) veins which drain the corpus cavernosum, penetrate the tunica albuginea and empty into the circumflex veins; these then drain into the deep dorsal venous system of the penis. The emissary veins may also drain directly into the deep dorsal vein. The superficial dorsal vein drains the distal portion of the corpora cavernosa, as well as the skin and glans. The deep and superficial dorsal veins can be routinely visualised by colour Doppler imaging in the midline of the penile shaft (Figs 12-3 and 12-4). The most proximal portions of the corpora cavernosa are drained by the cavernosal veins directly into the periprostatic venous plexus.4 FIGURE 12-3 Colour and spectral Doppler tracing of the normal dorsal penile vein. Note the uniform relatively slow velocity. When the penis is flaccid, its smooth muscle is in a tonic state, the cavernous sinusoids are collapsed, and the cavernous venules are open.2 The emissary veins drain the sinusoidal spaces and blood circulates into the dorsal veins. During this state, there is relatively high resistance to blood flow into the penis. Erection starts when an autonomic neurogenic impulse relaxes the cavernosal arterioles and sinusoidal spaces. As erection occurs, there is a marked increase in the volume of arterial inflow into the penis as the cavernous arteries dilate. This is accompanied by relaxation of the smooth muscle of the corpora cavernosa with expansion and elongation of the cavernous sinusoids as they fill with blood. Compression of the cavernous venules between the dilated cavernous sinusoids and the unyielding peripheral tunica albuginea decreases venous outflow. This veno-occlusive mechanism (which depends on neurological stimuli, a sufficient supply of arterial blood, and normal function of the tunica albuginea) maintains sinusoidal distension and rigid erection. Five stages of erectile physiology have been defined: latent, tumescent, full erection, rigid erection and detumescent. During the latent phase, the diameters of the cavernosal arteries are at their greatest and there is maximum inflow of blood with minimal resistance. During tumescence, the sinusoidal cavities of the corpora cavernosa distend with blood. With full erection, blood flow decreases, as do the diameters of the cavernosal arteries. With a rigid erection, blood inflow (and outflow) ceases and the diameters of the cavernosal arteries are at their narrowest. Detumescence occurs when the trabeculae and arteries contract in response to a release of norepinephrine. During the five stages of erection, different arterial diameters and waveform patterns are normally present on Doppler examination.5 The evaluation should be performed in a quiet, private setting with the room comfortably warm and darkened, so that the patient is relaxed and not uncomfortable. The scan is performed with the patient lying supine and the penis in the anatomical position (lying superiorly against the anterior abdominal wall). During the examination, the patient may be asked to help keep the penis immobilised by gently holding the corona just under the glans penis and then stretching the shaft along the anterior abdominal wall. Scanning is usually performed on the ventral surface of the penis, but the probe can be placed on the dorsal or lateral surfaces if necessary (Fig. 12-4). Imaging is performed in both the longitudinal and transverse planes from the base of the penis to the glans to visualise anatomical details of the corpora cavernosa, cavernosal arteries and surrounding structures, and also to demonstrate any abnormalities such as fibrosis, scarring, plaques, calcification, haematoma or tumour. The transducer should be applied gently with minimal penile compression. Firm pressure causing vascular compression can resist inflow and affect accuracy of velocity measurement, especially during diastole. The diameter of the arteries and blood flow velocities are measured. Colour Doppler enhances the accuracy of angle correction, which is mandatory for flow velocity determination. In addition, with colour Doppler, blood flow direction can be assessed and the presence of any communications between the cavernosal, dorsal and spongiosal arteries can be detected.6 The initial report of Doppler sonography combined with pharmacological induction of erection to evaluate vasculogenic impotence was by Lue and associates7 in the mid-1980s. The use of this study peaked before the introduction of phosphodiesterase inhibitors and has now fallen off significantly. Intra-cavernosal ejection of prostaglandin E1 at a dose of 10 μg into the base of the corpus cavernosum with a 27-gauge needle will result in an erection, even without sexual stimulation. If the response is sub-optimal the initial injection can be supplemented by a further 10 μg after 15 min. If the patient responds with an appropriate erection, then it can be presumed that neurogenic, psychogenic or hormonal issues are the cause of the patient’s erectile dysfunction. The Doppler examination of the cavernosal artery flow profile should be initiated within two minutes of injection. Reassessment is then performed every 2 to 5 minutes depending on the temporal response to the drug, which can vary considerably from patient to patient. Most examinations are finished by 20 minutes. Assessment up to 30 minutes is occasionally required to ensure the maximal pharmacologic effect has been attained. Doppler measurements are most reliable and most easily reproduced when taken at the base of the penis where the penile vessels angle posteriorly toward the perineum. The arterial diameter and waveform of each cavernosal artery is individually assessed. Peak systolic and end-diastolic velocities are measured and recorded. An asymmetric response of the cavernosal arteries during erection or a lack of arterial dilation may suggest the presence of a significant vascular inflow obstruction. The examiner should also carefully search for anatomical penile arterial variants as they may also contribute to vasculogenic impotence.8
Doppler Ultrasound of the Penis
Introduction
Penile Anatomy and Physiology
ARTERIAL ANATOMY
VENOUS ANATOMY
ERECTILE PHYSIOLOGY
Ultrasound Technique
Erectile Dysfunction
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Radiology Key
Fastest Radiology Insight Engine