Fig. 13.1
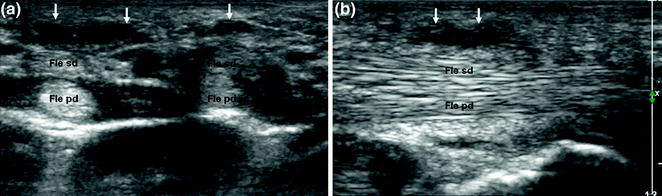
The palmar fascia (or aponeurosis) is composed of longitudinal fibers (mainly in the superficial portion) and transverse fibers (predominantly in deep layers). It is continuous with the flexor retinaculum and the palmaris longus tendons and covers the flexor tendons and the neurovascular structures of the palm
Dupuytren’s disease is characterized by nodular thickening and variable retraction of the palmar fascia [1, 2]. It is quite frequent in northern European populations, but rare in those of the Mediterranean area. Onset is more frequent after the age of 50, and there is a clear predilection for men (M/F ratio 7.6:1.0). Incidence rates are highest among individuals whose professions involve manual activities. The disease has been linked to a strong genetic predisposition that is transmitted in an autosomal dominant manner. Contrary to previous beliefs, the prevalence of Dupuytren’s disease is not increased in diabetics, smokers, alcoholics, or persons with epilepsy. It may be associated with other fibromatoses (Ledderhose’s disease, La Peyronie’s disease) [1, 4, 5].
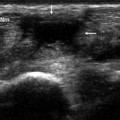
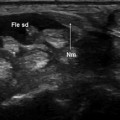
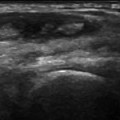
Clinically, Dupuytren’s disease presents with painless nodules and limited mobility of one or more fingers. Ultrasound imaging reveals hypoechoic nodules between the subcutaneous tissues and the flexor tendons (Figs. 13.2, 13.3). The nodules’ adherence to the flexor tendons can be demonstrated with dynamic studies. The role of sonography in this disease is to confirm the clinical diagnosis and characterize involvement of the flexor tendons. It can also be useful to guide local injection of drugs [6].