Fig. 7.1
The volar aspect of the wrist contains three tendons lying superficial to the carpal tunnel. The flexor carpi radialis (Frc), the palmaris longus (Pl), and the flexor carpi ulnaris (Fuc). a schematic diagram, b sonogram
The flexor carpi radialis is a long, cylindrical tendon that originates (via the common flexor tendon) on the medial epicondyle of the humerus and inserts into the bases of the second and third metacarpals [1]. It is surrounded by a synovial sheath that begins about 3 cm above the wrist and ends at the insertion. The most common disorder affecting the flexor carpi radialis is tenosynovitis, which is related to overuse, trauma or microtrauma, inflammatory diseases, and carpometacarpal arthropathy. It is manifested clinically by volar wrist pain at the level of the radius, often accompanied by local swelling. Based on the physical examination alone, synovitis of the flexor carpi radialis can be mistaken for a ganglion. The error can often be corrected by sonographic demonstration of the typical signs of synovitis (Fig. 7.2).
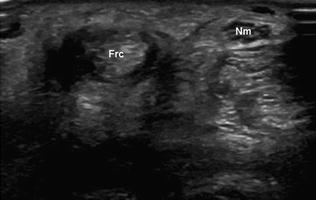
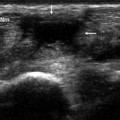
Fig. 7.2
Tenosynovitis of the flexor carpi radialis. Ultrasound reveals an anechoic peritendinous layer surrounding the flexor carpi radialis tendon (Frc)
The palmaris longus (together with the flexor carpi radialis and flexor carpi ulnaris) also originates on the medial epicondyle via the common flexor tendon. It normally consists of a small proximal muscle and a long, unsheathed distal tendon [2]. It runs through the superficial portion of the forearm between the radial (lateral) and ulnar (medial) flexors carpi, passing anterior to the flexor retinaculum (where some of its fibers insert) and continuing on to its distalmost insertion in the palmar fascia. It is well developed in mammals that use their anterior limbs to support the weight of their bodies and to walk, but in humans it is considered a nonessential accessory muscle.
For this reason, it is frequently used in tendon graft procedures. In humans, its main function is to maintain tension on the palmar fascia.
Anatomically, the palmaris longus is highly variable. Complete absence of the muscle and tendon (which has implications solely for reconstruction purposes) occurs in 15–20 % of the population, with substantial race-related variations in frequency [3]. The agenesis may be unilateral or bilateral. In the former case, it is usually confined to the nondominant hand [4]. A more clinically relevant variant is the reversed palmaris longus (Fig. 7.3). In this case, the proximal portion of the muscle that arises from the medial epicondyle is tendinous, while the belly of the muscle is located distally, attached to the palmar fascia. The reversal of these components often plays a role in carpal tunnel syndrome.

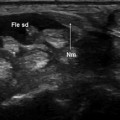
Fig. 7.3
Reversed palmaris longus. Ultrasound shows the belly (rather than the tendon) of the palmaris longus muscle overlying the carpal tunnel
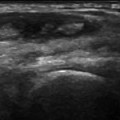
Lesions involving the palmaris longus are rare. Owing to the superficial course of the tendon, these lesions are usually the result of direct trauma (Fig. 7.4




Related posts:



Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
