Figure 29.1.1
Ectopic pregnancy with an extrauterine gestational sac containing a live embryo. A: Transvaginal view of the uterus and left adnexa demonstrates a gestational sac (calipers) containing an embryo (arrow), located between the uterus (UT) and left ovary (OV). B: The embryo (arrow) has cardiac activity, at a rate of 150 beats per minute, documented by M-mode.
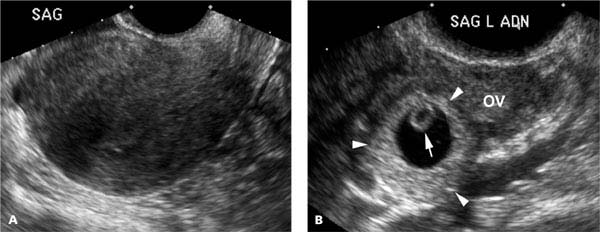
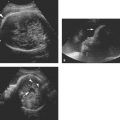
Figure 29.1.2
Ectopic pregnancy containing a yolk sac. A: Sagittal transvaginal view of the uterus shows no intrauterine gestational sac. B: In the left adnexa adjacent to the ovary (OV) is a gestational sac (arrowheads), containing a yolk sac (arrow).
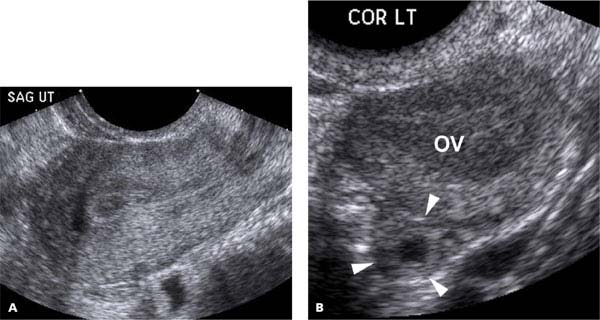
Figure 29.1.3
Ectopic pregnancy with an adnexal tubal ring. A: Sagittal transvaginal view of the uterus shows no intrauterine gestational sac. B: In the left adnexa adjacent to the ovary (OV) is a fluid collection with a thick echogenic rim (arrowheads), termed a “tubal ring”.
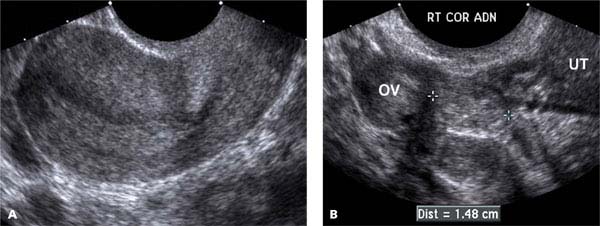
Figure 29.1.4
Ectopic pregnancy with an adnexal mass. A: Sagittal transvaginal view of the uterus shows no intrauterine gestational sac. B: In the right adnexa between the ovary (OV) and the uterus (UT) is an adnexal mass (calipers), representing the ectopic pregnancy.
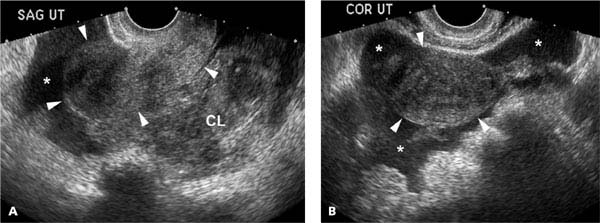
Figure 29.1.5
Ectopic pregnancy with free intraperitoneal fluid. A: Sagittal and (B) coronal transvaginal views of the pelvis in a woman with a positive pregnancy test demonstrate a large amount of free fluid (*) surrounding the uterus (arrowheads) and ill-defined material, representing blood clot (CL), in the cul-de-sac. No intrauterine gestational sac is seen.
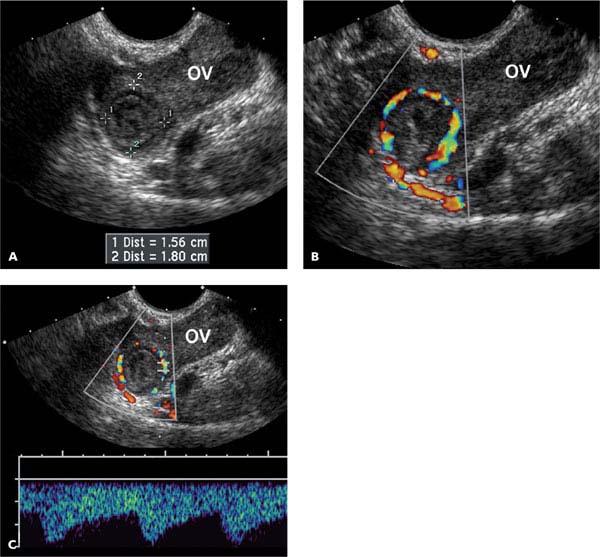
Figure 29.1.6
Ectopic pregnancy with adnexal mass: Doppler findings. A: Coronal transvaginal view through the left adnexa demonstrates a complex mass (calipers) adjacent to the ovary (OV). B: Color Doppler demonstrates that the mass has prominent blood flow surrounding it (sometimes termed “ring of fire”). C: Spectral Doppler waveform from the periphery of the mass demonstrates a large amount of blood flow at end-diastole, indicative of low impedance flow.
29.2. Cornual (Interstitial) Ectopic Pregnancy
Description and Clinical Features
Cornual ectopic pregnancy is one that implants in the interstitial portion of the fallopian tube, the part of the tube that traverses the cornu of the uterus. This is an uncommon form of ectopic pregnancy but, like other ectopics, occurs more frequently in pregnancies achieved via assisted reproductive techniques than those achieved naturally.
A gestational sac in the cornu can grow for a period of time, but the cornu has a far more limited ability to expand than does the body of the uterus. Once the cornu has reached its maximal size, further sac growth will lead to cornual rupture and potentially life-threatening bleeding. Fortunately, pain usually occurs earlier than rupture, so prompt diagnosis when the patient presents with symptoms can save the patient’s life or spare her from a hysterectomy. Ultrasound-guided ablation is one of the treatment options.
Sonography
On ultrasound, cornual ectopic pregnancy appears as a gestational sac located in the superolateral portion of the uterus, separate from but contiguous with the body of the uterus, bulging the external uterine contour. Little or no myometrium is seen around the lateral or superior aspect of the gestational sac (Figures 29.2.1 to 29.2.3). A high volume of blood flow may be seen around the sac on color Doppler (Figures 29.2.2 and 29.2.3).
Distinguishing between cornual ectopic pregnancy and an eccentrically located intrauterine gestation (e.g., a gestational sac in one horn of a bicornuate uterus) can present a diagnostic dilemma. Because the management of these two entities is markedly different—cornual ectopic pregnancy requires emergent treatment and an eccentrically placed intrauterine gestational sac requires no treatment—it is extremely important to be accurate in distinguishing between them. While the conventional sonographic features described above are generally sufficient to establish the diagnosis, 3D ultrasound with a true coronal view of the uterus can be useful by providing a clear depiction of the body and cornu of the uterus (Figure 29.2.3).
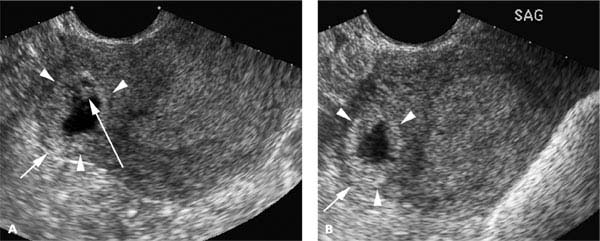
Figure 29.2.1
Cornual ectopic pregnancy with a live embryo at 6 weeks gestation. A: Coronal and (B) sagittal transvaginal views of the uterus reveal a gestational sac (arrowheads) in the right superolateral aspect of the uterus, a region corresponding to the right cornu. The sac bulges the external contour of the uterus and there is little or no hypoechoic myometrium around the bulging portion of the sac (short arrow). The gestational sac contains an embryo (long arrow), and cardiac activity was seen on real-time sonography.
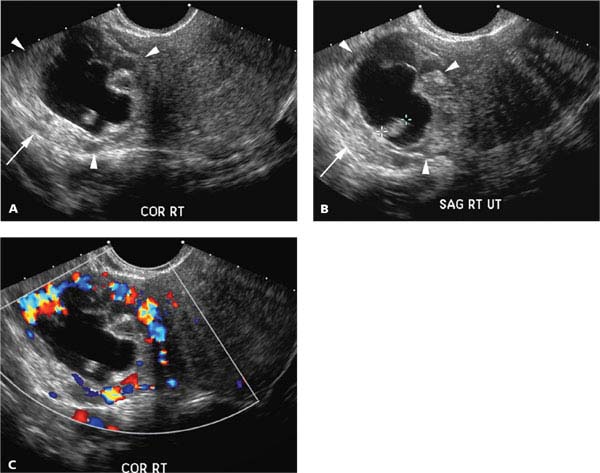
Figure 29.2.2
Cornual ectopic pregnancy with extensive blood flow. A: Coronal and (B) sagittal transvaginal views of the uterus reveal a large gestational sac (arrowheads) in the right superolateral aspect of the uterus, a region corresponding to the right cornu. The sac bulges the external contour of the uterus and there is little or no hypoechoic myometrium around the bulging portion of the sac (arrow). The gestational sac contains an embryo (calipers). C: Color Doppler reveals extensive blood flow around the periphery of the sac.
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


