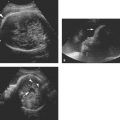
Figure 23.1.1
Intravascular blood transfusion into the umbilical vein at its placental insertion. A: Using ultrasound, a needle (arrowheads) was guided to place its tip into the umbilical vein. B: Blood is seen streaming (arrowheads) from the tip of the needle (arrow) into the vein.
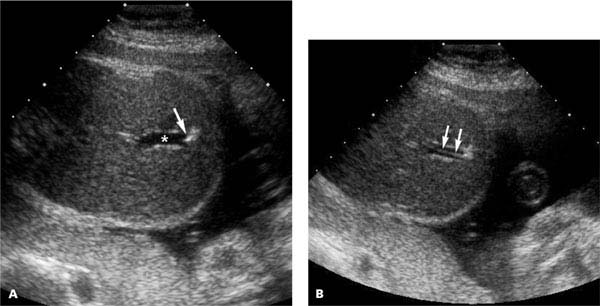
Figure 23.1.2
Intravascular blood transfusion into the intrahepatic umbilical vein. A: Transverse section through the fetal abdomen demonstrates the tip of a needle (arrow) within the intrahepatic umbilical vein (*). B: There is streaming of blood (arrows) as it is transfused into the umbilical vein.

Figure 23.1.3
Intraperitoneal blood transfusion. A needle (arrowheads) traverses the fetal abdominal wall and ends in fluid (*) within the abdomen that accumulated from the transfusion as blood was injected through the needle.
23.2. Thoracentesis and Thoracoamniotic Shunting
Description and Clinical Features
Drainage of fetal pleural effusions may improve pregnancy outcome in a number of situations. Examples include the following:
Hydrops with a large unilateral pleural effusion: drainage of the unilateral effusion may increase venous return to the fetal heart by correcting mediastinal shift, thereby improving or alleviating hydrops.
Large bilateral pleural effusions in a fetus immediately before delivery: bilateral thoracenteses, followed immediately by delivery, will allow the neonatal lungs to expand and obviate the need for emergency postnatal thoracenteses.
Fluid may be removed by thoracentesis, whereby a needle is inserted into the fetal thorax, fluid is aspirated, and the needle is removed. In some cases with hydrops, thoracentesis may provide only temporary improvement, after which the pleural effusion recurs and the hydrops persists or worsens. If this happens, placing a thoracoamniotic shunt may be necessary, to provide continuous drainage of the pleural fluid.
Sonography
Fetal thoracentesis is performed using real-time sonographic monitoring to guide a needle into the fetal thorax (Figure 23.2.1). Placement of a thoracoamniotic shunt involves several steps, all directed by ultrasound (Figure 23.2.2). First, a large-bore needle is directed into the fetal thorax. The trocar is removed and a double-pigtail catheter is threaded through the needle until one end of the catheter coils in the fetal thorax. The needle is then pulled back until its tip is in the amniotic fluid, and the remaining part of the catheter is pushed out of the needle into the amniotic cavity. The needle is then withdrawn to complete the procedure.
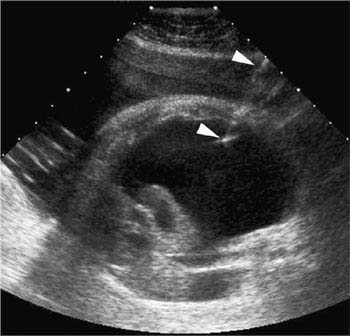
Figure 23.2.1
Fetal thoracentesis. A needle (arrows), inserted percutaneously through the maternal anterior abdominal wall, ends in the thorax of a fetus with a large pleural effusion.
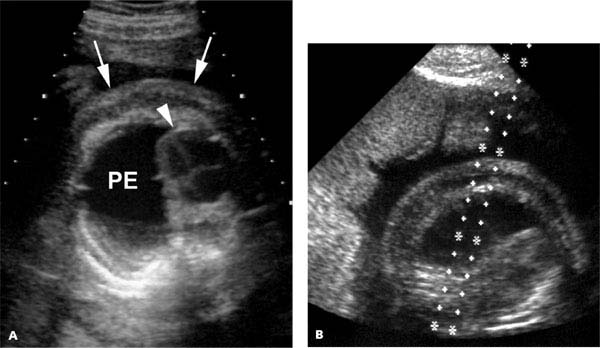
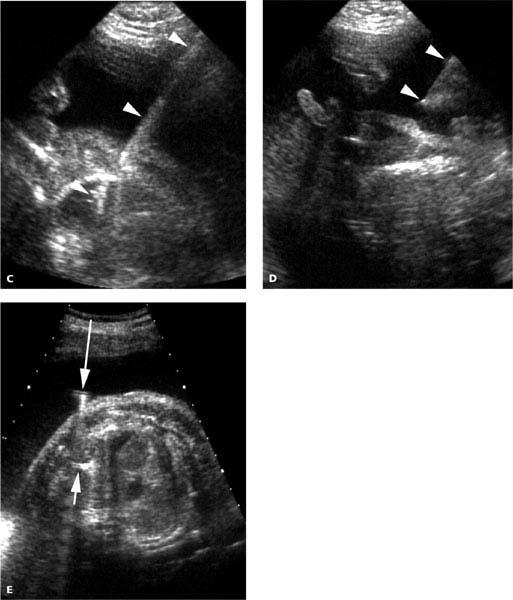
Figure 23.2.2
Thoracoamniotic shunt placement. A: Transverse section of the fetal thorax reveals a large left-sided pleural effusion (PE) deviating the heart (arrowhead) to the right. Subcutaneous edema (arrows) is seen around the thorax. B: In preparation for thoracentesis, a needle guide was placed on the transducer and guide marks on the image indicate the path that a needle inserted through the guide will follow. C: A needle (arrowheads) traverses the amniotic fluid and ends within the pleural effusion in the fetal thorax. D: After one end of a double-pigtail catheter was inserted into the fetal thorax, the needle (arrowheads) was withdrawn into the amniotic fluid. E: At the conclusion of the procedure, one end of the shunt catheter is seen in the amniotic fluid (long arrow) and the other within the fetal thorax (short arrow).
23.3. Bladder Drainage and Vesicoamniotic Shunting
Description and Clinical Features
Urethral obstruction, which is most commonly due to posterior urethral valves, is likely to cause life-threatening pulmonary hypoplasia from severe, prolonged oligohydramnios and renal dysplasia from urinary obstruction. Both of these serious complications of urethral obstruction can sometimes be treated in utero by ultrasound-guided percutaneous placement of a vesicoamniotic shunt, which provides relief of the urinary obstruction by diverting urine from the bladder to the amniotic cavity, in the process replenishing amniotic fluid volume.
A fetus diagnosed with urethral obstruction must meet several criteria before a corrective procedure should be considered:
Severe oligohydramnios: in the absence of severe oligohydramnios, the prognosis is good without surgery because bladder outlet obstruction is incomplete.
Gestational age incompatible with viability outside the uterus.
No other major structural anomaly.
Normal karyotype.
Renal parenchyma appears normal on ultrasound.
Normal fetal renal function: if the above criteria are met, fetal renal function is evaluated by performing an ultrasound-guided fetal bladder drainage. The presence of normal fetal urinary electrolyte levels and reaccumulation of urine in the fetal bladder over the next 24 hours indicate adequate renal function.
If all these criteria are met, in utero treatment of the urethral obstruction should be contemplated.
Sonography
Ultrasound plays a central role in all aspects of the diagnosis and treatment of urethral obstruction, including diagnosing the condition, assessing whether the fetus is a candidate for in utero intervention, and guiding the drainage procedure and placement of the vesicoamniotic shunt. After the diagnosis is established by ultrasound, ultrasound is used to assess the amniotic fluid volume, evaluate the fetal renal parenchyma for evidence of dysplasia (parenchymal cysts or thin echogenic cortex), conduct a comprehensive fetal anatomic survey to assess for coexisting anomalies, assign gestational age, and guide amniocentesis or umbilical blood sampling to determine fetal karyotype. If the assessment finds no contraindication to proceeding, ultrasound is then used to guide a needle into the fetal urinary bladder (Figure 23.3.1) to assess renal function.
When the decision is made to proceed with vesicoamniotic shunting, shunt placement is performed under ultrasound guidance (Figure 23.3.2). The procedure often begins with an amnioinfusion (reverse amniocentesis): instillation of saline into the amniotic space to create a pocket of fluid in which to place the amniotic end of the vesicoamniotic shunt. A large-bore needle is then inserted into the fetal bladder and a double-pigtail catheter is inserted through the needle. One end of the catheter is advanced into the fetal bladder. The needle is then withdrawn into the amniotic fluid, and the rest of the catheter is pushed out of the needle, so that the second coil of the catheter is in the amniotic cavity. The needle is then removed.
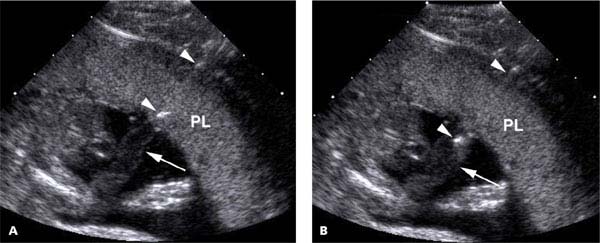
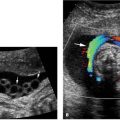
Figure 23.3.1
Fetal bladder drainage. A: A needle (arrowheads) has been guided by ultrasound into a distended fetal bladder (*). B: After urine has been withdrawn, the bladder (*) is considerably smaller.
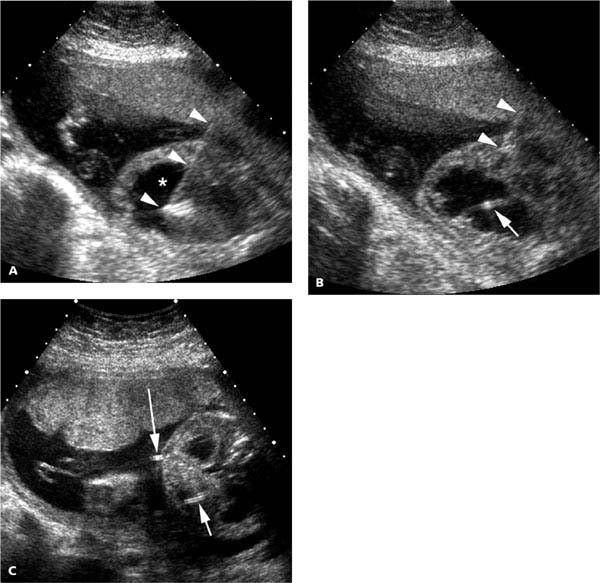
Figure 23.3.2
Vesicoamniotic shunt placement. A: A needle (arrowheads) has been inserted into the distended fetal bladder (*). B: A catheter (arrow) has been advanced into the bladder, and the needle (arrowheads) is being withdrawn out of the fetus. At this point, the other end of the catheter lies within the needle, to be pushed out of the needle when the needle tip is pulled back into the amniotic fluid. C: At the end of the procedure, one end of the catheter is in the fetal bladder (short arrow) and the other end is in the amniotic fluid (long arrow).
Once a shunt has been placed, the fetus should be monitored closely by ultrasound. If the shunt is working properly, the fetal bladder will remain decompressed. Redistention of the bladder indicates shunt malfunction, due to either debris clogging the shunt or dislodgment of the shunt, which necessitates either delivery of the fetus or insertion of a new shunt.
23.4. Paracentesis
Description and Clinical Features
Fetal ascites is often seen as a component of hydrops. It can also occur in other settings, such as urine ascites in a fetus with calyceal rupture due to urinary tract obstruction. In most cases of fetal ascites, there is no benefit to performing prenatal paracentesis. Occasionally, however, removing the fluid can improve the outcome (e.g., decreasing abdominal girth at term to permit vaginal delivery or relieving upward pressure on the diaphragm to facilitate lung growth).
Sonography
Fetal paracentesis is performed under continuous ultrasound guidance (Figures 23.4.1 and 23.4.2). The needle is advanced through the maternal abdominal and uterine walls and directed toward a site on the fetal abdominal wall overlying a pocket of ascites. When the needle is in an appropriate location adjacent to the fetal abdomen and there is no fetal motion, the needle is quickly advanced through the abdominal wall into the ascites.
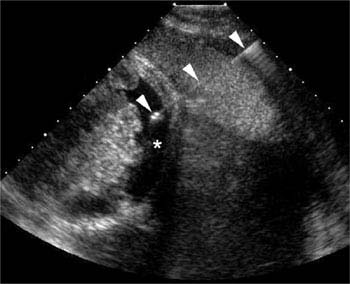
Figure 23.4.1
Fetal paracentesis with a small-to-moderate amount of ascites. A needle (arrowheads), inserted percutaneously through the maternal anterior abdominal wall, ends in the abdomen of this fetus with ascites (*).
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


