Abstract
Elevation of the diaphragm may be the result of low lung volume, but apparent asymmetric elevation of a hemidiaphragm requires an explanation and may be the result of abdominal diseases, asymmetric loss of lung volume, pleural effusion, diaphragmatic hernias, phrenic nerve paralysis, or even diaphragmatic or pleural tumors.
Keywords
atelectasis, Bochdalek, hypoplastic lung, phrenic nerve paralysis, Morgagni, subpulmonic pleural effusion, traumatic diaphragmatic hernias
Questions
- 1.
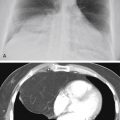
Which one the following diagnoses is most likely in the case illustrated in Fig. 6.1 ?
- a.
Hepatomegaly.
- b.
Interposition of the colon.
- c.
Right upper lobe atelectasis.
- d.
Phrenic nerve paralysis.
- e.
Right upper lobe pneumonia.

Fig. 6.1
- a.
- 2.
Which of the following is least likely to be associated with pleural effusion?
- a.
Primary lung tumor.
- b.
Interposition of colon.
- c.
Subphrenic abscess.
- d.
Echinococcal cyst.
- e.
Metastasis.
- a.
- 3.
Which of the following is not true of phrenic nerve paralysis?
- a.
Results in complete loss of motion of the diaphragm at fluoroscopy.
- b.
May be secondary to primary lung tumor in the apex.
- c.
May be secondary to mediastinal malignant tumor.
- d.
Occasionally is idiopathic.
- e.
Results in paradoxic motion of the diaphragm.
- a.
Discussion
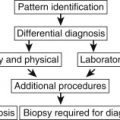
Elevation of the diaphragm offers a variety of radiologic challenges ( Chart 6.1 ). When both sides of the diaphragm are symmetrically elevated, the differential is significantly different from that with unilateral elevation. The most common cause of elevation of both sides of the diaphragm is failure of the patient to inspire deeply. This is frequently voluntary, but may be an indicator of a significant pathologic process. Obesity is probably the most common abnormality resulting in low lung volume. A similar appearance may be produced by a variety of abdominal conditions, including ascites and large abdominal masses. Bilateral atelectasis may also result in the elevation of both sides of the diaphragm, but is usually identifiable by increased opacity in the lung bases. Restrictive pulmonary diseases may likewise result in elevation of both sides of the diaphragm (see Cicatrizing Atelectasis in Chapter 13 ).
- I.
Subpulmonic pleural effusion 32 , 53
- II.
Abdominal disease
- A.
Subphrenic abscess
- B.
Distended stomach
- C.
Interposition of the colon
- D.
Liver mass (e.g., tumor, abscess, echinococcal cyst)
- A.
- III.
Decreased lung volume
- A.
Atelectasis
- B.
Postoperative lobectomy and pneumonectomy
- C.
Hypoplastic lung
- A.
- IV.
Phrenic nerve paralysis
- A.
Primary lung cancer
- B.
Malignant mediastinal tumor
- C.
Iatrogenic
- D.
Idiopathic
- A.
- V.
Diaphragmatic hernia 336 (e.g., foramina of Morgagni and Bochdalek)
- VI.
Eventration of the diaphragm
- VII.
Traumatic rupture of the diaphragm
- VIII.
Diaphragmatic tumor (e.g., lipoma, 153 fibroma, mesothelioma, metastasis, lymphoma)
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


