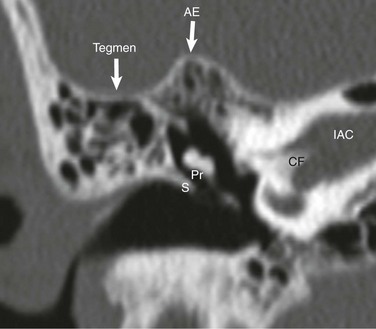
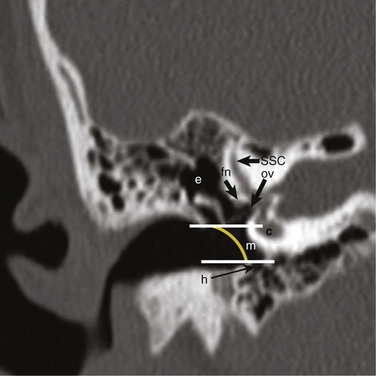
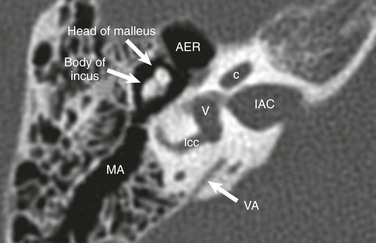
Chapter 9 The pinna (auricle) develops from six mesenchymal proliferations, called hillocks, which are located at the dorsal ends of the first and second pharyngeal arches. They surround the first pharyngeal cleft (the future external auditory meatus). These hillocks gradually fuse and form the definitive auricle.1 The tympanic cavity is derived from endoderm and develops from the first pharyngeal pouch. This pouch grows laterally until it comes in contact with the floor of the first pharyngeal cleft. The lateral part of the pouch gives rise to the primitive tympanic cavity. The medial part of the pouch is smaller and forms the eustachian tube. The malleus and incus are derived from the cartilage of the first pharyngeal arch, whereas the stapes is derived from the second pharyngeal arch. The ossicles remain embedded in the mesenchyme until the eighth month, when the surrounding tissue dissolves. The tympanic cavity expands dorsally to form the mastoid antrum late during fetal life. Pneumatization of the mastoid process continues after birth.1 Between the sixth and eighth weeks of gestation, the cochlear duct, arising from the saccule, penetrates the surrounding mesenchyme and completes the two and a half turns. The thin residual connection between the cochlea and saccule is the ductus reuniens. At the tenth week, the cartilage that differentiated from the mesenchyme surrounding the cochlear duct undergoes vacuolization and two perilymphatic spaces are formed: the scala tympani and the scala vestibuli. The cochlear duct (scala media) is separated from the scala vestibuli by the vestibular membrane and from the scala tympani by the basilar membrane. The lateral wall of the cochlear duct remains attached to the surrounding cartilage by the spiral ligament. Medially, the cochlear duct is attached to the modiolus, which is the axis of the bony cochlea. At 6 weeks gestation, semicircular canals appear as outpouchings of the utricular (posterior) component of the otic vesicle.1 The temporal bone consists of tympanic, squamous, petrous, and mastoid parts and a styloid process.2 The temporal bone may be divided into compartments when studying its anatomy or reviewing imaging studies. These compartments are described from lateral to medial. Detecting subtle abnormalities of the pinna with imaging may be difficult, but in general it is possible to identify gross malformations or absence of pinna on CT. Ossicular abnormalities are present in 98% of the temporal bones with microtia and external auditory canal (EAC) abnormality.3 In cross section, the EAC is oval in shape. Its walls (anterior and posterior; superior and inferior) run parallel to each other throughout the course of the EAC. The EAC consists of two segments: a membranous (fibrocartilaginous) segment that makes up the lateral third of the EAC, and a medial bony segment that forms the remainder of it.4 The tympanic membrane separates the EAC from the middle ear cavity and is attached to the tympanic annulus, which is a circumferential bony prominence at the medial-most aspect of the bony EAC. Superiorly, the tympanic membrane attaches to the scutum (e-Fig. 9-1), which is an important bony landmark in the diagnosis and evaluation of cholesteatoma. If the tympanic membrane is not thickened, wide window settings on CT are required to visualize it. The tympanic cavity is an aerated space medial to the tympanic membrane. Air reaches the middle ear cavity from the nasopharynx via the eustachian tube. The middle ear cavity is arbitrarily divided into three compartments: epitympanum (attic), mesotympanum, and hypotympanum. With lines drawn parallel to the superior and inferior walls of the bony segment of the EAC on the coronal plane, the part of the middle ear cavity above the upper line is the epitympanum (attic), which is the largest portion and houses the bulk of the ossicular chain. The mesotympanum lies between the two lines. The hypotympanum is below the lower line and normally is nonexistent or very small in children (Fig. 9-2). The malleus, incus, and stapes form the ossicular chain, which is responsible for amplification (~30%) and transmission of sound waves from the tympanic membrane to the oval window on the vestibule.5 The manubrium (handle) and the lateral process of the malleus are embedded in the tympanic membrane. The tympanic membrane has two parts, divided by the lateral process of the malleus: a smaller pars flaccida superiorly, and a larger pars tensa inferiorly.6 Cranial to the manubrium is the neck of the malleus, to which the tendon of the tensor tympani muscle attaches. The tensor tympani muscle is derived from the first branchial arch and is innervated by the only branch of the trigeminal nerve that has motor fibers: V3 (mandibular branch). The head of the malleus forms the “ice cream” of the familiar “ice cream and cone” appearance and articulates with the body of the incus (Fig. 9-3). The malleoincudal joint is a diarthrodial (synovial) articulation, as is the incudostapedial joint (Figs. 9-3 and 9-4). Figure 9-3
Embryology, Anatomy, Normal Findings, and Imaging Techniques
Embryology
External Ear
Middle Ear
Inner Ear
Anatomy and Normal Findings
Pinna and External Auditory Canal
Middle Ear Cavity (Cleft)
Ossicles
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree