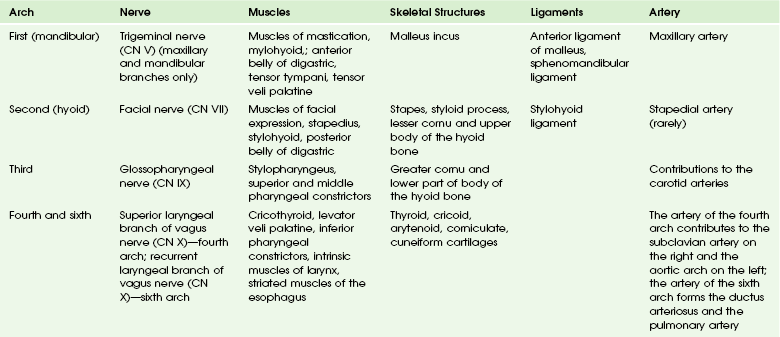
Chapter 13 This chapter will focus on the embryology of the neck and the oral cavity. The embryology of the orbit, face and sinuses, temporal bone, and ear are addressed in Chapters 4, 8, 9, and 18. The mesenchyme is derived from three main sources: 1. The lateral plate mesoderm, which forms the laryngeal cartilages and regional connective tissue 2. The neural crest cells, whose migration initiates the formation of the pharyngeal arch skeletal structures and regional bone, cartilage, tendons, and glandular stroma 3. The ectodermal placodes, from which originate the fifth, seventh, ninth, and tenth cranial nerves (CNs) After neurulation occurs, the mesoderm subdivides into the lateral, intermediate, and paraxial mesoderm. The lateral mesoderm forms most of the throat and larynx. The intermediate mesoderm does not form any part of the head and neck. The paraxial mesoderm forms the seven somitomeres and 42 to 44 paired somites. The five most rostral somites are involved in the formation of head and neck musculature (Fig. 13-1). The somitomeres and somites form before the development of the branchial apparatus. Figure 13-1 Embryology. The contribution of the somitomeres and somites to the formation of muscles and their distinct innervation is unchanged throughout growth and development. Thus although many muscles migrate in location, their nerve supply is maintained and hence their branchial arch origin can always be identified (see Fig. 13-1). Branchial Arches: The first branchial arch (Fig. 13-2) is composed of a dorsal segment known as the maxillary process and a ventral segment known as Meckel cartilage or the mandibular process; both involute. The ossification around Meckel cartilage is the precursor of the mandible and the sphenomandibular cartilage in the neck. The muscle derivatives of the first arch are the muscles of mastication (the masseter, pterygoid, and temporalis muscles), the tensor tympani and tensor veli palatine muscles, the anterior belly of the digastric muscle, and the mylohyoid muscle. The trigeminal nerve (CN V) provides motor and sensory innervation to the first branchial arch. Figure 13-2 Embryology. Branchial Pouches: The first branchial pouch does not contribute to the structures of the neck. The second branchial pouch gives rise to the palatine tonsils and tonsillar fossa. The third branchial pouch gives rise to the inferior parathyroids and thymus. The early embryologic connections to the pharynx normally are obliterated. The fourth branchial pouch gives rise to the superior parathyroid glands and the ultimobranchial body, which contains the parafollicular cells (C cells) of the thyroid gland. The fifth branchial pouch degenerates. The branchial clefts do not contribute to any neck structures and are obliterated as development occurs (Tables 13-1 and 13-2). Table 13-1 Derivatives of the Branchial Arches Adapted from Moore KL, Persaud MG, Torchia MG. Before we are born. Philadelphia: Saunders/Elsevier; 2008. Table 13-2 Derivatives of the Branchial Pouches
Embryology, Anatomy, Normal Findings, and Imaging Techniques
Embryology of the Neck
Development of the Mesenchyme
Development of the Mesoderm, Somitomeres, and Somites
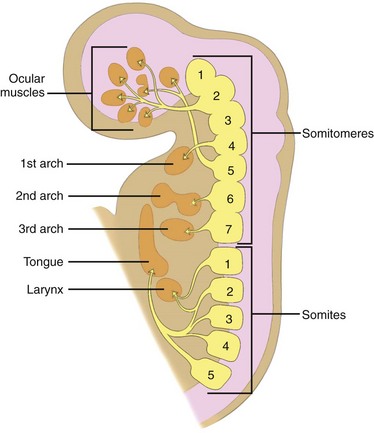
A sagittal section shows the relationship of somitomeres and somites and their corresponding derivatives. (From Som P, Curtin H. Head and neck imaging. 4th ed. Philadelphia: Mosby; 2003.)
Development of the Branchial Apparatus
Branchial Apparatus and its Contribution to the Structures of the Neck
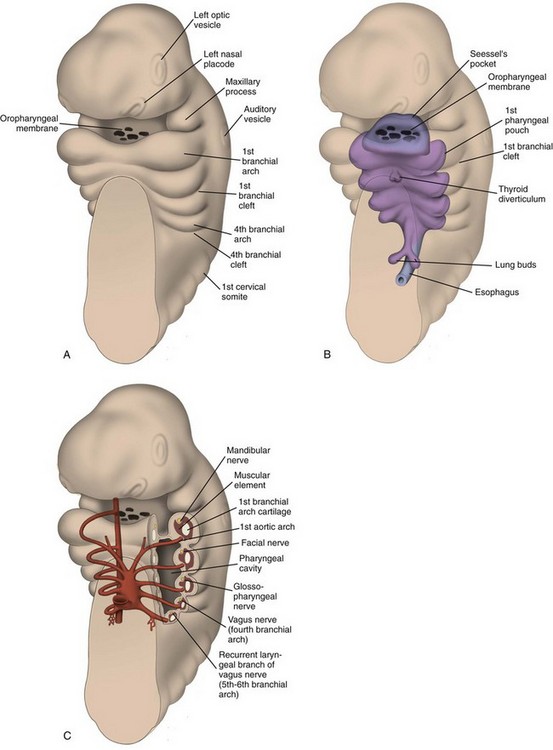
Relationship of branchial arches and clefts and subsequent derivative structures. (From Som P, Curtin H. Head and neck imaging. 4th ed. Philadelphia: Mosby; 2003.)
Pouch
Derivatives
First
Eustachian tube, middle ear, portions of mastoid bone
Second
Palatine tonsils, tonsillar fossa
Third
Inferior parathyroids, thymus
Fourth and sixth
Superior parathyroids, parafollicular cells of thyroid Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access