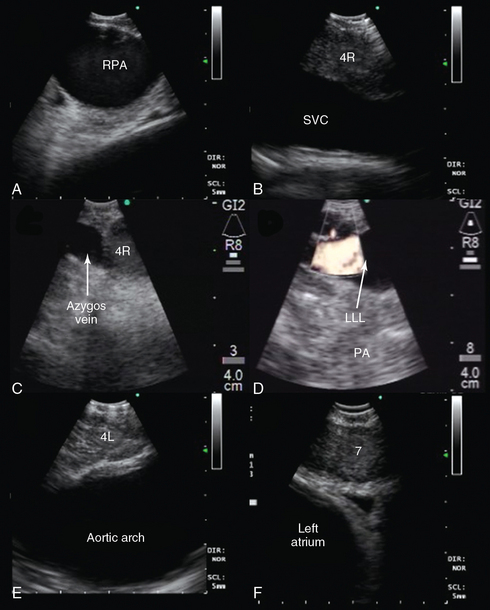
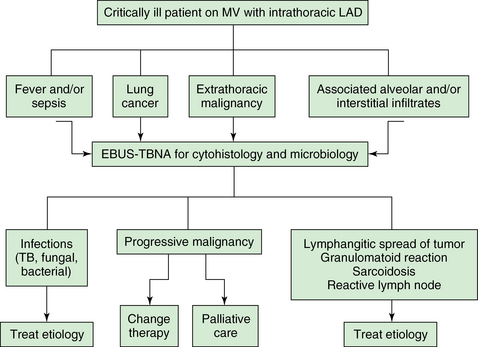
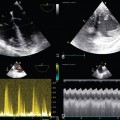
25 Convex probe endobronchial ultrasound-guided transbronchial needle aspiration is used for diagnosing (and staging) intrathoracic lymphadenopathy in lung cancer,1 other intrathoracic tumors,2 and lymphadenopathy from extrathoracic malignancies.3 The aspiration yield for benign causes of intrathoracic lymphadenopathy is less than with cancer, mostly because of lack of tissue architecture in cytology specimens, but sarcoidosis, and bacterial, mycobacterial, and fungal infections can be diagnosed.4–6 High-frequency endobronchial ultrasound (EBUS), using a radial scanning probe, is used to diagnose peripheral pulmonary nodules7 and to define airway wall structures in tracheal stenosis, tracheobronchomalacia, excessive dynamic airway collapse, and tumor invasion.8–10 Extraluminal vascular structures (superior vena cava, azygos vein, main pulmonary artery and its branches, ascending and descending aorta, aortic arch, pulmonary veins, and left atrium) are visualized using convex probe EBUS (see Figure 25-5 in the imaging case box). Bronchoscopists can assess volume status, pericardial fluid, or the presence of pulmonary embolism.11,12 Thoughtful resource use for intensive care unit (ICU) admissions13 warrants that EBUS should be considered in critically ill patients with suspected lung, mediastinal, cardiovascular, and hemodynamic disorders. This chapter illustrates potential applications of EBUS and EBUS–transbronchial needle aspiration (TBNA) in patients admitted to the ICU or undergoing general anesthesia. Moreover, we suggest algorithms built on the strengths of EBUS diagnostic abilities, its minimally invasive nature, and its proven safety profile for the noncritically ill patient setting (based on our own institutional experience). Figure 25-5 Convex probe endobronchial ultrasound (EBUS) visualization of mediastinal vascular structure. After introduction of the bronchoscope via the endotracheal tube (ETT), the right lower lobe bronchus is approached. The transducer is turned 90 degrees to the lateral wall to visualize the right lower lobe pulmonary artery (PA). Pulling back the bronchoscope, the take-off of the middle lobe PA is examined. With the transducer oriented anteriorly, the right pulmonary artery (RPA) is visualized crossing the right main bronchus (A), and the right upper lobe PA take-off is seen if the transducer is oriented anterolaterally near the main carina. After turning the bronchoscope medially, the pulmonary trunk is inspected. Above the RPA, with the transducer oriented anterolateral and pulled back, the superior vena cava (SVC) is examined (B). Continuing to turn the bronchoscope laterally, the azygos vein is visualized (C). The investigation of the left side also starts in the lower lobe bronchus after turning the bronchoscope to the lateral wall to visualize the left lower lobe (LLL) PA (D) and, after pulling back the bronchoscope and orienting it anteromedial, the left upper lobe PA. The left PA is visualized behind the lateral wall of the left main bronchus up to the left lower paratracheal region; continuing to pull back and orient the transducer laterally, the aortic arch is encountered (E). Subcarinal region with pulmonary veins and left atrium is visualized either from the left or right main bronchi when the transducer is oriented medially (F). Many patients admitted to the ICU demonstrate enlarged intrathoracic lymph nodes on computed tomography (CT) scans performed for a variety of reasons. Sampling lymph nodes could assist in management. For example, patients with hypoxemic respiratory failure and parenchymal or interstitial infiltrates may have associated lymphadenopathy of variable significance. Although a patient with pneumonia likely has reactive lymphadenopathy, needle aspiration could reveal the actual organism. Patients with sarcoidosis and anthracosis have characteristic findings on EBUS-TBNA specimens (granulomatous reaction and anthracotic histiocytes, respectively).4,14 EBUS-TBNA can make the diagnosis of primary lung cancer or extrathoracic malignancy, metastatic to mediastinal, and hilar lymph nodes. It allows staging or restaging of patients with known or suspected malignancy.1–3 This information is used to redefine level of care, ICU priority scores, and guide treatment. A patient with cancer on mechanical ventilation, for example, may be at risk for transbronchial or transthoracic lung biopsies. EBUS-TBNA can make a diagnosis of progressive disease, infections, or granulomatoid reaction (Figure 25-1). Figure 25-1 Proposed algorithm for using (convex probe) endobronchial ultrasound (EBUS) in critically ill patients with intrathoracic lymphadenopathy. A No. 8.5 to 9 endotracheal tube (ETT) is used to facilitate passage of the EBUS bronchoscope (outer diameter [OD], 6.9 mm) and prevent auto–peak end-expiratory pressure (PEEP). LAD, Lymphadenopathy; MV, mechanical ventilation; TB, tuberculosis; TBNA, transbronchial needle aspiration. Extrinsic compression is often amenable to interventional procedures, such as airway stent insertion,15 so that patients with respiratory failure on mechanical ventilation may be weaned from ventilators.16 Bronchoscopy and EBUS-TBNA are performed for the dual purpose of diagnosing the central airway obstruction (CAO) (Figure 25-2) and making a cytohistologic diagnosis by sampling impinging masses. Doppler mode is useful to assess the vascularity of the mass and suggests tumor engorgement with potential worsening airway obstruction in the supine position or hypervolemic state. A rapid diagnosis allows prompt referral for stent insertion and systemic therapy. A patient with a large mediastinal cyst could even be drained17 rather than be referred for open surgery. Figure 25-2 Potential role of endobronchial ultrasound (EBUS) in critically ill patients with mediastinal masses (arrows). A, Large pretracheal mass compressing the lower trachea and main carina. B, Near-complete obstruction in the lower trachea and proximal mainstem bronchi because of extrinsic compression and excessive dynamic airway collapse. C, Large (3 cm in anteroposterior diameter), heterogeneous mass confirmed to be small cell lung cancer (SCLC) on rapid on-site cytology examination (ROSE). D, Proposed use of EBUS and white light bronchoscopy (WLB) in patients with mediastinal masses requiring mechanical ventilation. CTX, Chemotherapy; EBRT, external beam radiotherapy; MV, mechanical ventilation; PA, pulmonary artery; PAH, pulmonary arterial hypertension; SVC, superior vena cava; TBNA, transbronchial needle aspiration; *Tracheal wall invasion by a primary lung tumor defines a T4 and thus at least stage IIIB lung cancer. Expiratory central airway collapse (ECAC) is a reported cause of hypercarbic respiratory failure as well as inability to wean from mechanical ventilation. Diagnosis can be made with white light bronchoscopy (WLB), but assessment of airway wall structures requires visualization in cross section (Figure 25-3
Endobronchial ultrasound
(CONSULTANT-LEVEL EXAMINATION)
Overview
Intrathoracic lymphadenopathy
Extrinsic central airway obstruction, pulmonary artery compression, and superior vena cava syndrome
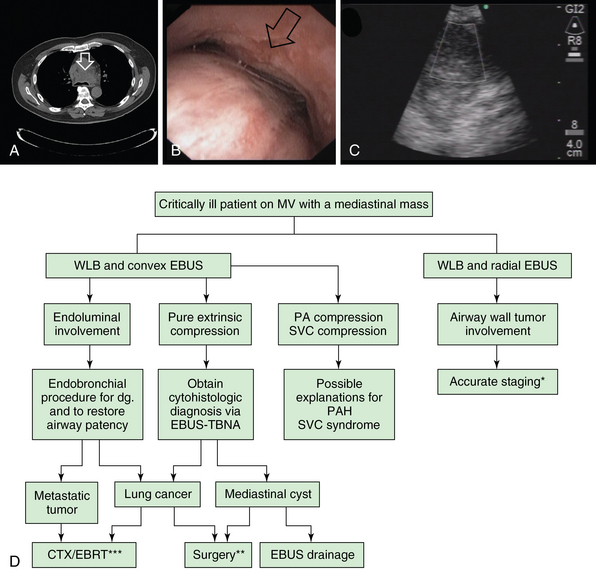
** Surgical treatment is considered for cases of large mediastinal cysts compressing the airway and not treatable by other minimally invasive techniques. For lung cancer, surgery is considered if the tumor is deemed resectable after complete staging AND if the patient is operable. ***In general, CTX and EBRT are offered once patient’s functional status improves after liberation from mechanical ventilation.
Expiratory central airway collapse, tracheal stenosis, and airway wall tumor invasion
Related posts:
 Ultrasound-guided peripheral intravenous access
Ultrasound-guided peripheral intravenous access
 Ultrasound-guided arterial catheterization
Ultrasound-guided arterial catheterization
 Ultrasound-guided placement of inferior vena cava filters: (CONSULTANT-LEVEL EXAMINATION)
Ultrasound-guided placement of inferior vena cava filters: (CONSULTANT-LEVEL EXAMINATION)
 Ultrasonography in circulatory failure
Ultrasonography in circulatory failure
 Evaluation of right ventricular function in the intensive care unit by echocardiography: (CONSULTANT-LEVEL EXAMINATION)
Evaluation of right ventricular function in the intensive care unit by echocardiography: (CONSULTANT-LEVEL EXAMINATION)
 Procedural ultrasound for surgeons: (CONSULTANT-LEVEL EXAMINATION)
Procedural ultrasound for surgeons: (CONSULTANT-LEVEL EXAMINATION)
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Radiology Key
Fastest Radiology Insight Engine
