Fig. 16.1
Epidemic parotitis. (a) Plain CT scanning demonstrates swollen and enlarged right parotid gland with uneven density. (b, c) Contrast CT scanning demonstrates uneven enhancement of the right parotid gland
Case Study 1
A female patient aged 64 years had a history of parotitis for over 1 month. She had symptoms of swelling and pain at the anterior lower part of the right ear, and her symptoms are relieved after receiving anti-infection therapy.
16.7.2 Epidemic Parotitis-Related Complications
16.7.2.1 Neurological Complications
Encephalitis
The radiological demonstrations are not characteristic. CT scanning and MR imaging demonstrate no abnormalities in mild cases. CT scanning commonly demonstrates cerebral white matter edema. Plain CT scanning demonstrates low-density lesions and poorly defined interface between the gray and white matter. Contrast CT scanning demonstrates no enhancement of the lesions. MR imaging demonstrates the lesions having long T1 long T2 signals in the caudate nucleus, lenticular nucleus, anterior limb of internal capsule, thalamus, midbrain, and cerebellar hemispheres (Fig. 16.2). DWI demonstrates limited diffusion of the lesions (Fig. 16.3).
Fig. 16.2
Epidemic parotitis complicated by encephalitis. (a) On admission, MRI T2WI demonstrates multiple patches of high-signal shadows in bilateral frontal lobes. (b) Reexamination 20 days after her admission demonstrates increased quantity of lesions, indicating progress of the conditions (Reprint with permission from Sonmez et al. 2004)
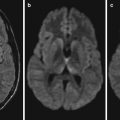
Fig. 16.3
Epidemic parotitis complicated by encephalitis. (a–c) At day 4 after admission, MRI T1WI, T2WI, and FLAIR demonstrate no cerebellar lesions. (d–e) At day 10 after admission, DWI and ADC demonstrate symmetrically limited diffusion of bilateral cerebellum (arrowhead). (f) DWI demonstrates no abnormal signals of the cerebellum (Reprint with permission from Matsukuma et al. 2008, 29)
Case Study 2
A girl patient aged 4 years was diagnosed with parotitis. At week 1 after the onset, she experienced fever, conscious change, left facial paralysis, and abduct nerve paralysis. She began to show ataxia and dysphonia 20 days after her admission.
Case Study 3
A boy patient aged 5 years was diagnosed with epidemic parotitis. He had symptoms #of high fever, headache, vomiting, and cervical rigidity for 3 days. CT scanning demonstrates no abnormalities.
Hydrocephalus
CT scanning and MR imaging demonstrate symmetrical dilation of cerebral ventricles, smaller brain parenchyma, and no accompanying widened and deepened sulci and gyri.
Case Study 4
A boy aged 8 years had symptoms of fever, headache, vomiting, and ataxia. Laboratory tests show cerebrospinal fluid protein, 122.8 mg/L; glucose, 3.219 mmol/L; and increased cells count that are predominantly lymphocytes. CT scanning demonstrates dilated 3rd and 4th ventricles.
For case detail and figures, please refer to from Aydemir C. Pediatr Neurosurg, 2009, 45(6): 419.
Myelitis
The radiological demonstrations are not characteristic. MR imaging demonstrates swollen and thickened segmental spinal cord, with equal or low signal by T1WI and high signal by T2WI. Contrast MR imaging demonstrates no abnormal enhancement of lesions or small nodules or patches of enhancement. In some cases, enhancement of spinal pia mater can be demonstrated.
Case Study 5
A male patient aged 22 years had symptoms of conscious changes, respiratory distress, dyspraxia, and urine retention 2 weeks after the onset.
For case detail and figures, please refer to Unal A. Spinal Cord, 2005, 43(7): 441.
Deafness
MRI T2WI demonstrates abnormal signals in the inner ear. 3D-FLAIR demonstrates nodular high-signal shadows in the cochlea and vestibule (Fig. 16.4).
Fig. 16.4
Epidemic parotitis complicated by deafness. (a) Transverse MRI 3D-FLAIR demonstrates nodular high-signal shadows (pointed by arrow) in the right cochlea and vestibule. (b, c) Plain T1WI and T2WI demonstrate no sign of lesions (Reprint with permission from Otake et al. 2006)
Case Study 6
A boy patient aged 6 years had a history of contact to patients with EP. By examinations and tests, increased IgM and IgG antibodies, intact bilateral tympanic membrane, deafness on the right ear, and normal hearing on the left ear are evident.
16.7.2.2 Digestive Complications
Pancreatitis
Ultrasound
Ultrasound demonstrates diffusive enlargement of the pancreas with poorly defined boundary and decreased/increased parenchymal echo with homogeneous or heterogeneous distribution.
CT Scanning
CT scanning demonstrates diffusive enlargement of the volume of the pancreas with poorly defined boundary, normal or slightly lower density of the pancreas that is homogeneous or heterogeneous, slight dilation of the pancreatic duct, and possibly accompanying peripancreatic effusion or ascites (Fig. 16.5). Contrast CT scanning demonstrates homogeneously enhanced pancreas with no necrotic area.

Fig. 16.5
Epidemic parotitis complicated by pancreatitis. CT scanning demonstrates slightly enlarged volume of the parotid gland with even density and rough edge, no dilated pancreatic duct, and drainage tube shadow in the stomach and duodenum
Case Study 7
A female patient aged 16 years complained of upper abdominal pain, nausea, and vomiting for 2 days, with accompanying poor appetite. She had a history of epidemic parotitis. By laboratory test, blood amylase is 656 U/L.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


