1
Esophagus
Esophageal Carcinoma
Overview
 Adenocarcinoma
Adenocarcinoma
• Most common esophageal cancer in the United States
• More common in the lower third of the esophagus
 Squamous cell carcinoma
Squamous cell carcinoma
• Most common esophageal cancer worldwide
• More common in the upper third of the esophagus
Risk Factors
 Tobacco use
Tobacco use
 Heavy alcohol use
Heavy alcohol use
 Barrett esophagus
Barrett esophagus
 Caustic injury
Caustic injury
Signs and Symptoms
 Dysphagia and odynophagia
Dysphagia and odynophagia
 Weight loss
Weight loss
 Midsternal chest pain
Midsternal chest pain
 Hoarseness of voice
Hoarseness of voice
 Early esophageal cancer is usually asymptomatic
Early esophageal cancer is usually asymptomatic
Diagnosis
 Esophagogram
Esophagogram
 Endoscopy with biopsy
Endoscopy with biopsy
 Endoscopic ultrasound for staging purposes-assess the depth of invasion and involvement of regional nodes
Endoscopic ultrasound for staging purposes-assess the depth of invasion and involvement of regional nodes
 Bronchoscopy to assess for airway invasion
Bronchoscopy to assess for airway invasion
 CT of the chest, abdomen, and pelvis for staging purposes
CT of the chest, abdomen, and pelvis for staging purposes
 PET scan to evaluate local and distant metastasis
PET scan to evaluate local and distant metastasis
Treatment
 Depending on the stage of the disease, treatment may include surgery, chemotherapy, and radiation therapy
Depending on the stage of the disease, treatment may include surgery, chemotherapy, and radiation therapy
 Advanced disease with dysphagia—may palliate symptoms with esophageal stent placement, laser therapy, or electrocoagulation
Advanced disease with dysphagia—may palliate symptoms with esophageal stent placement, laser therapy, or electrocoagulation
KEY POINT
 Remember that the esophagus has no serosal layer, so invasion to adjacent structures (trachea, aorta, pericardium) is common
Remember that the esophagus has no serosal layer, so invasion to adjacent structures (trachea, aorta, pericardium) is common
RADIOLOGY
 Plain film findings
Plain film findings
• Air-fluid level within the superior mediastinum with widening of the azygoesophageal line
 Esophagram findings
Esophagram findings
• Focal strictures with irregular borders/abrupt shoulder margins
• Can also appear as long tubular filling defects similar to esophageal varices, but do not change with patient positioning
• There may be stiffening of the mucosa and failure to collapse completely after the peristaltic wave passes, unlike achalasia
• In contrast, leiomyomas and gastrointestinal stromal tumors (GISTs) are smooth wide-based, submucosal filling defects that form obtuse angles with the normal esophagus
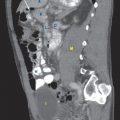
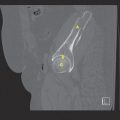
 CT findings (Fig. 1.1)
CT findings (Fig. 1.1)
• Mainly used in the staging of esophageal cancer
 Mediastinal lymphadenopathy
Mediastinal lymphadenopathy
 Effacement of the surrounding mediastinal fat, representing local invasion
Effacement of the surrounding mediastinal fat, representing local invasion
• Although nonspecific, there may be thickening of the esophageal wall
• Dilated esophagus cranial to the lesion due to obstruction
 PET/CT findings
PET/CT findings
• Hypermetabolic soft tissue within the esophagus
• More sensitive and specific than CT in identifying lymphadenopathy and overall staging
 Endoscopic US findings
Endoscopic US findings
• Carcinoma appears as a hypoechoic mass which interrupts the layers of the esophageal wall
FIGURE 1.1 A,B
A. Vertebra
B. Descending aorta
C. Heart
D. Stomach
E. Small bowel loops
F. Psoas muscle

FIGURE 1.1 A




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


