2
Hernias
Hernias occur when there is an anatomical defect or an area that is weakened, allowing abdominal contents such as small bowel, omentum, etc. to herniate.
KEY POINTS
 The most significant consequence of a hernia is incarceration of the herniated viscera that may lead to strangulation
The most significant consequence of a hernia is incarceration of the herniated viscera that may lead to strangulation
 Strangulation may lead to bowel necrosis and is therefore a surgical emergency
Strangulation may lead to bowel necrosis and is therefore a surgical emergency
• Skin changes (redness) overlying the area of incarceration, severe tenderness, leukocytosis, and signs of sepsis are classical signs for strangulation
 Hernias with a small neck have increased risk of incarceration and strangulation compared to larger neck hernias
Hernias with a small neck have increased risk of incarceration and strangulation compared to larger neck hernias
Incisional/Ventral Hernias
 Risk factors include previous abdominal surgeries, obesity, smoking, steroid usage
Risk factors include previous abdominal surgeries, obesity, smoking, steroid usage
 Diagnosed when the hernia occurs in the vicinity of a prior incision
Diagnosed when the hernia occurs in the vicinity of a prior incision
RADIOLOGY
Abdominal Incisional Hernia
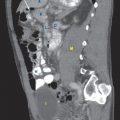
 CT findings (Fig. 2.1)
CT findings (Fig. 2.1)
• Can occur within any part of the abdominal wall
• Displacement of abdominal contents through the abdominal wall defect
FIGURE 2.1 A–C
A. Small bowel loops
B. Psoas muscle
C. Vertebra
D. Liver
E. Descending aorta
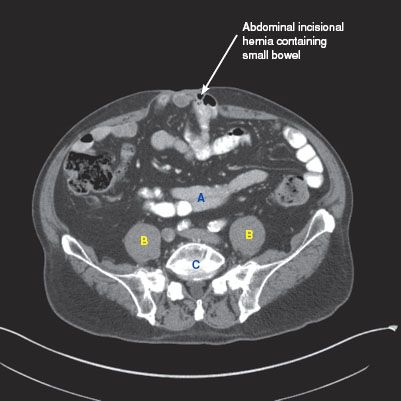
FIGURE 2.1 A
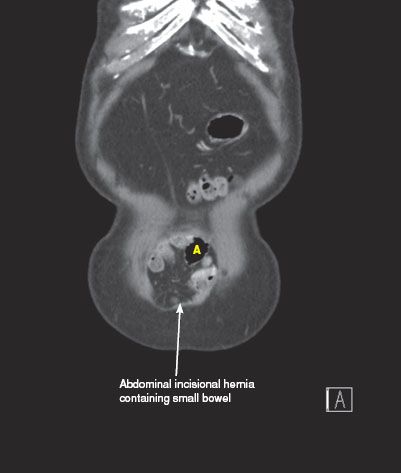
FIGURE 2.1 B

FIGURE 2.1 C
Incisional Hernia with Acutely Incarcerated Bowel—Dilated and Thickened
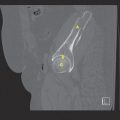
 CT findings (Fig. 2.2)
CT findings (Fig. 2.2)
• Thickened, edematous bowel loops with or without dilated proximal loops indicating obstruction
• Fat stranding may be noted in the mesentery within the incisional hernia, indicating venous congestion or inflammation
• Incarceration is suggested when herniation is associated with thickened bowel loops within the hernia with or without dilated bowel loops located proximal to the hernia
FIGURE 2.2 A–C
A. Rectum
B. Bladder
C. Small bowel loops
D. Vertebra
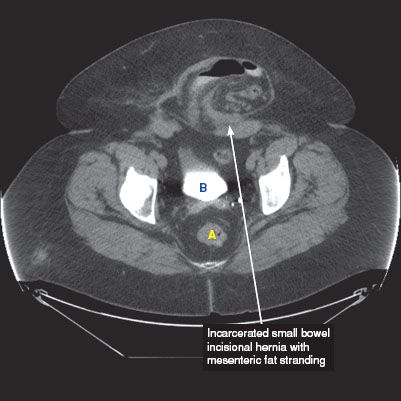
FIGURE 2.2 A
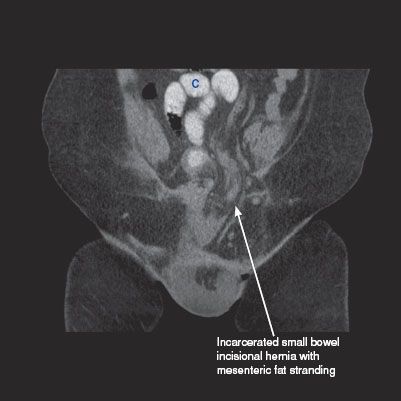
FIGURE 2.2 B

FIGURE 2.2 C
Status Post Ventral Hernia Repair
 CT findings (Fig. 2.3)
CT findings (Fig. 2.3)
• Depending on how the repair was performed, the postoperative abdomen will contain either:
 Staples which are small hyperdensities with streak artifact
Staples which are small hyperdensities with streak artifact
 Polypropylene (PP) mesh which are not usually visualized because its density is similar to soft tissue
Polypropylene (PP) mesh which are not usually visualized because its density is similar to soft tissue
 Polytetrafluoroethylene (PTFE) mesh which appear as linear areas of high density
Polytetrafluoroethylene (PTFE) mesh which appear as linear areas of high density
FIGURE 2.3 A–C
A. Liver
B. Gallbladder
C. Kidney
D. Vertebra
E. Small bowel loops
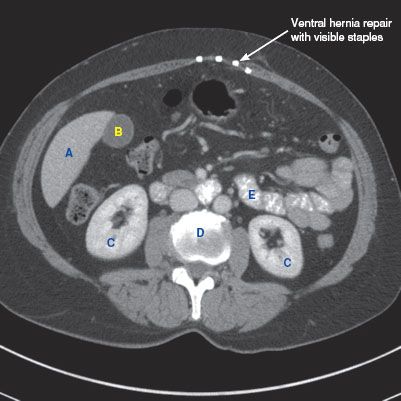
FIGURE 2.3 A
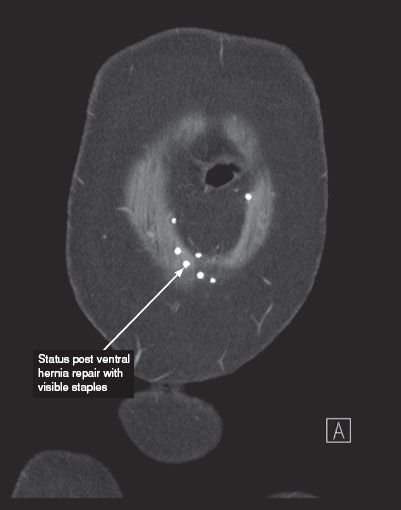
FIGURE 2.3 B
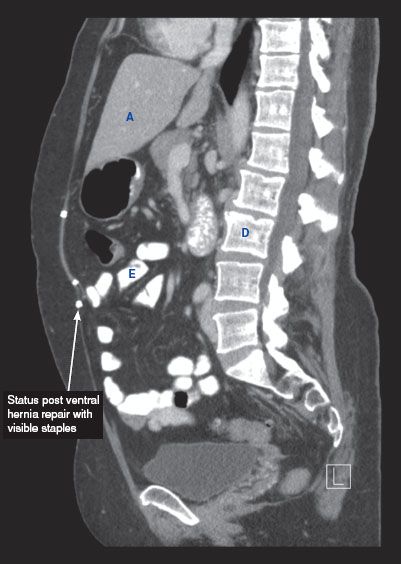
FIGURE 2.3 C
Status Post Ventral Hernia Repair—Infected Mesh with Abscess
 CT findings (Fig. 2.4)
CT findings (Fig. 2.4)
• Fluid or phlegmon adjacent to the site of the hernia repair
• Because superficial fluid collections are usually treated conservatively, superficial collections must be differentiated from deep collections
• Gas or septa may develop in a fluid collection
• Aspiration of fluid collection is often need to make the diagnosis
FIGURE 2.4 A,B
A. Small bowel loops

FIGURE 2.4 A
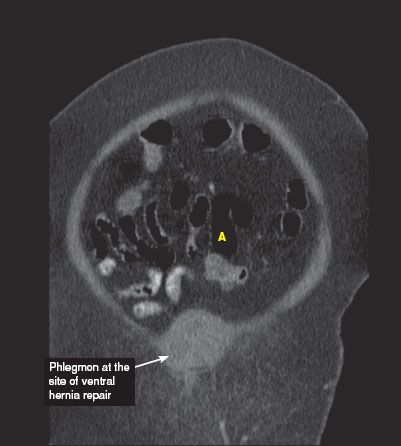
FIGURE 2.4 B
Flank Incisional Hernia
 CT findings (Fig. 2.5)
CT findings (Fig. 2.5)
• Protrusion of mesentery, bowel loops, or other abdominal organs through the lateral abdominal wall defect
FIGURE 2.5 A,B
A. Kidney
B. Small bowel
C. Vertebra
D. Liver
E. Iliopsoas muscle

FIGURE 2.5 A




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


