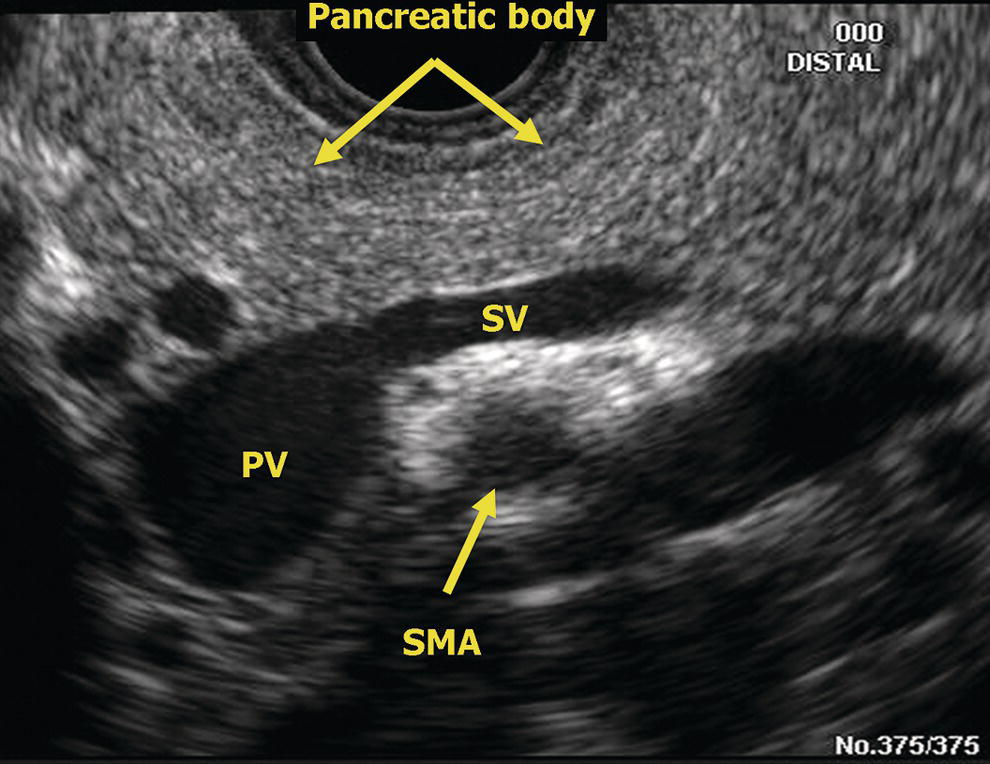
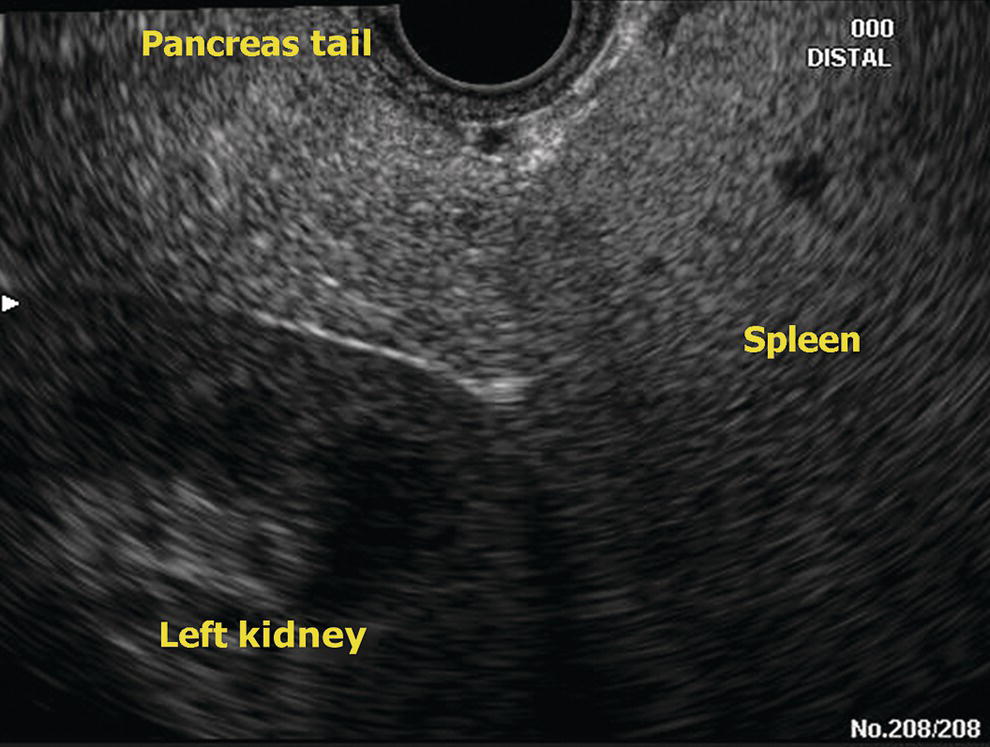
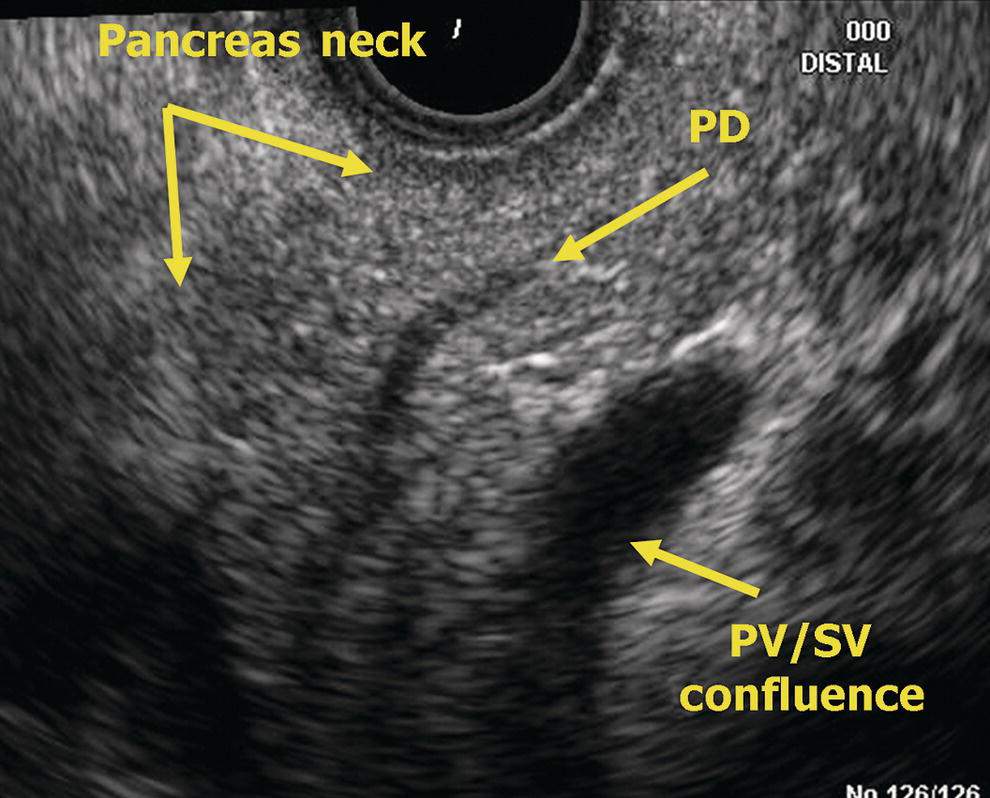
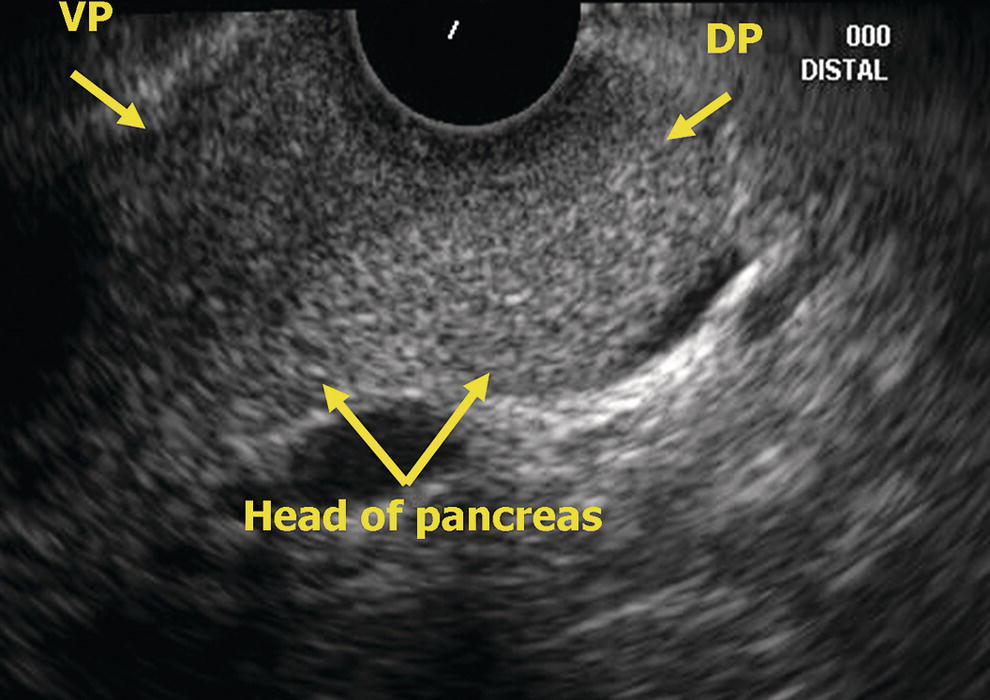
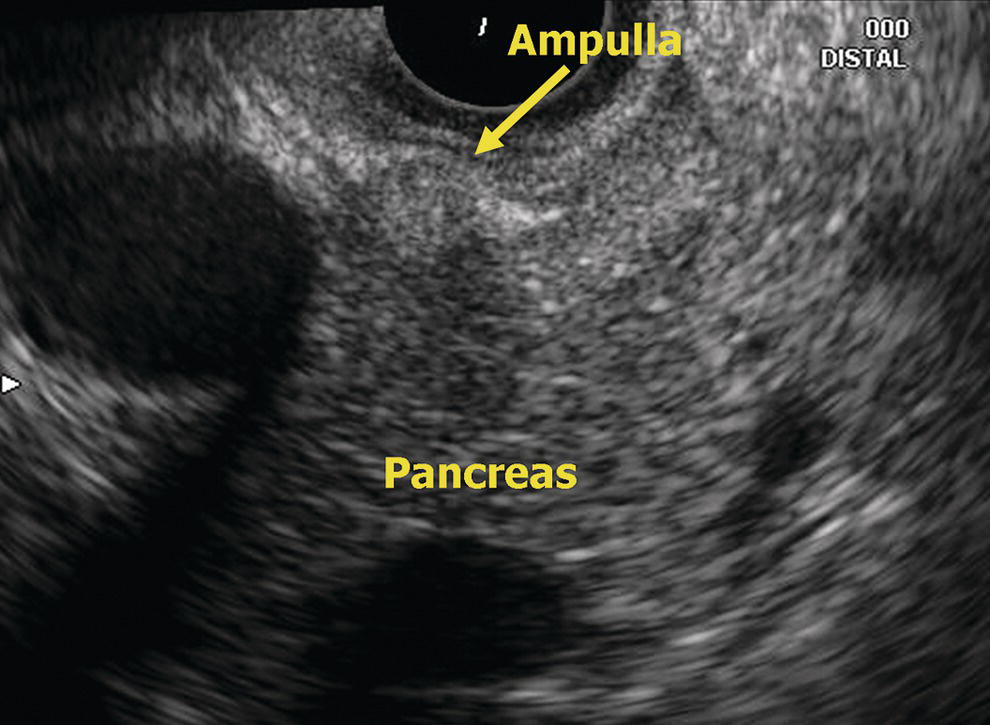
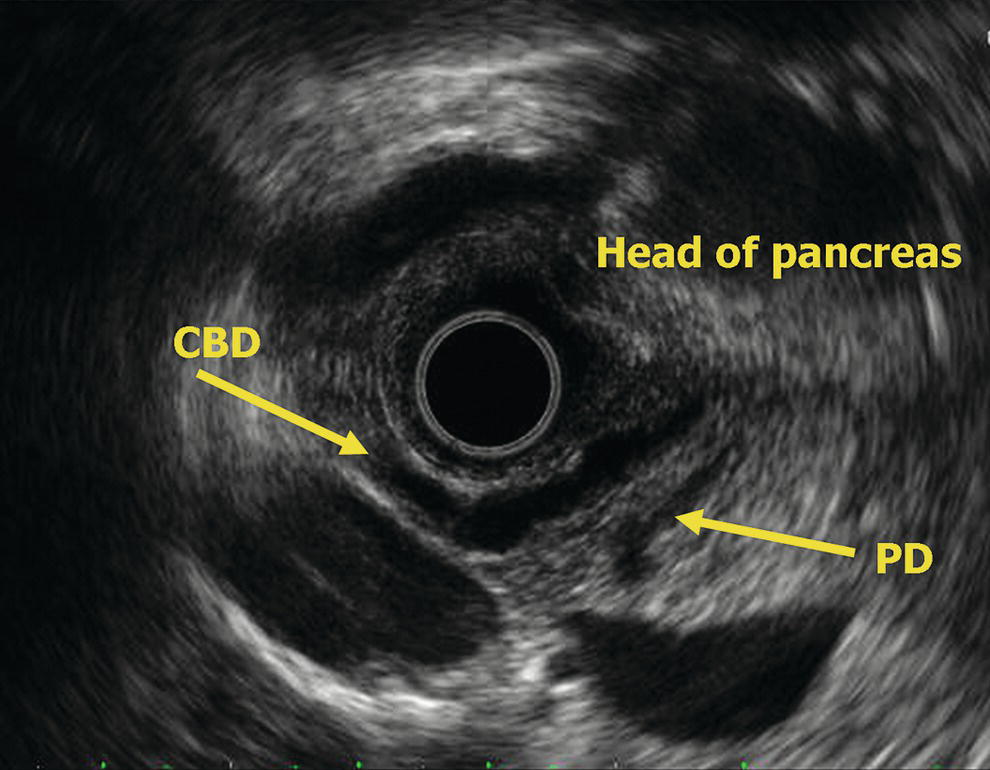
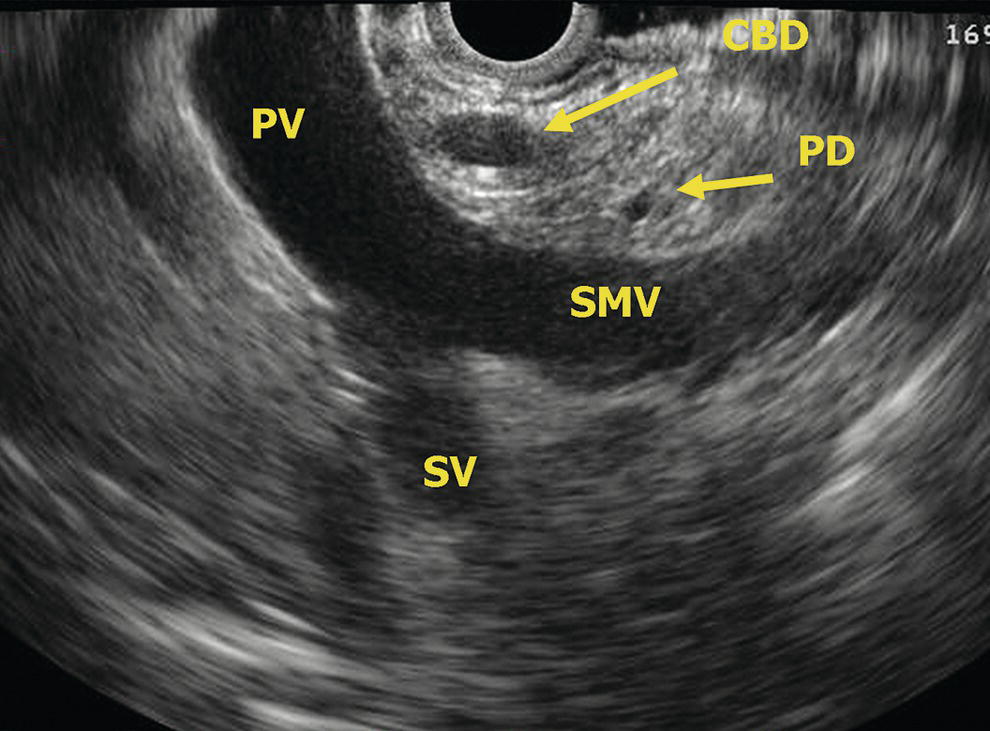
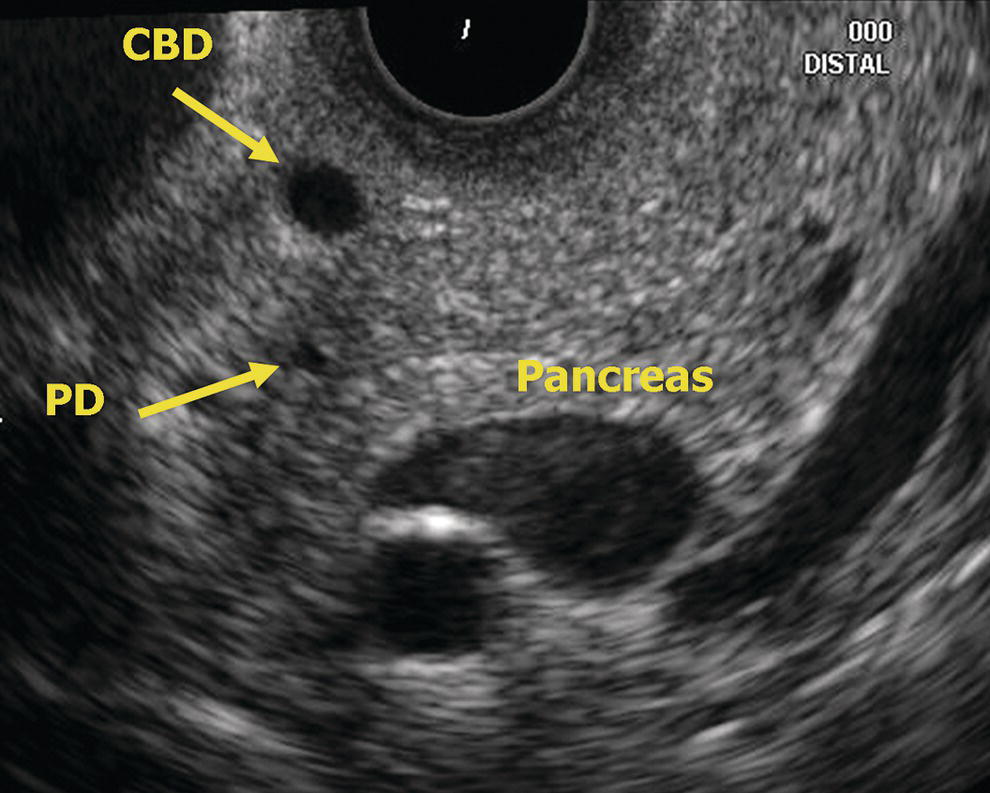
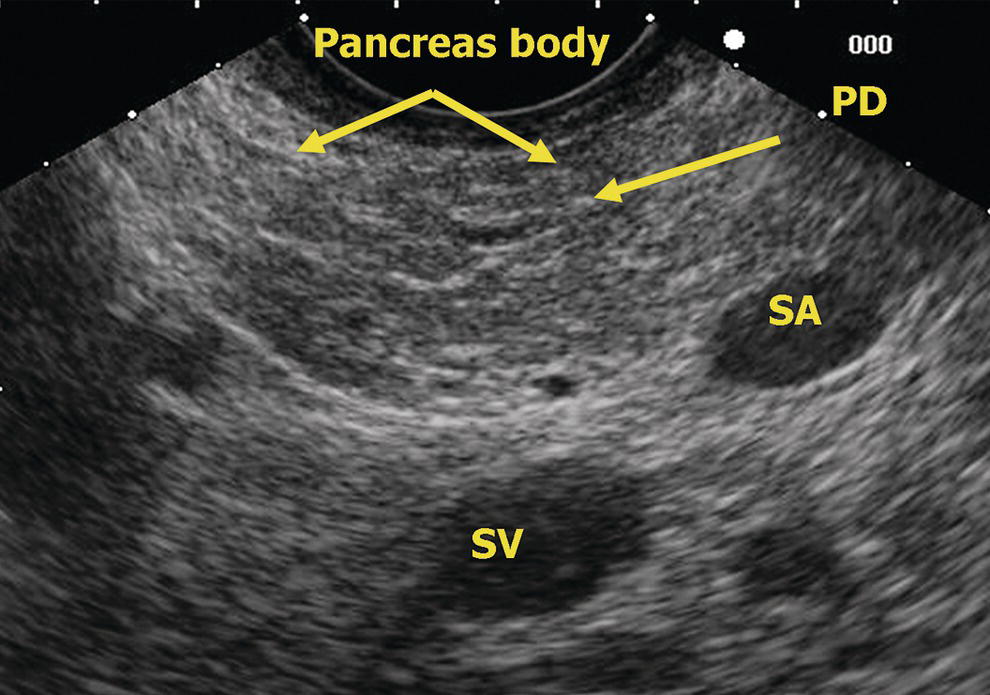
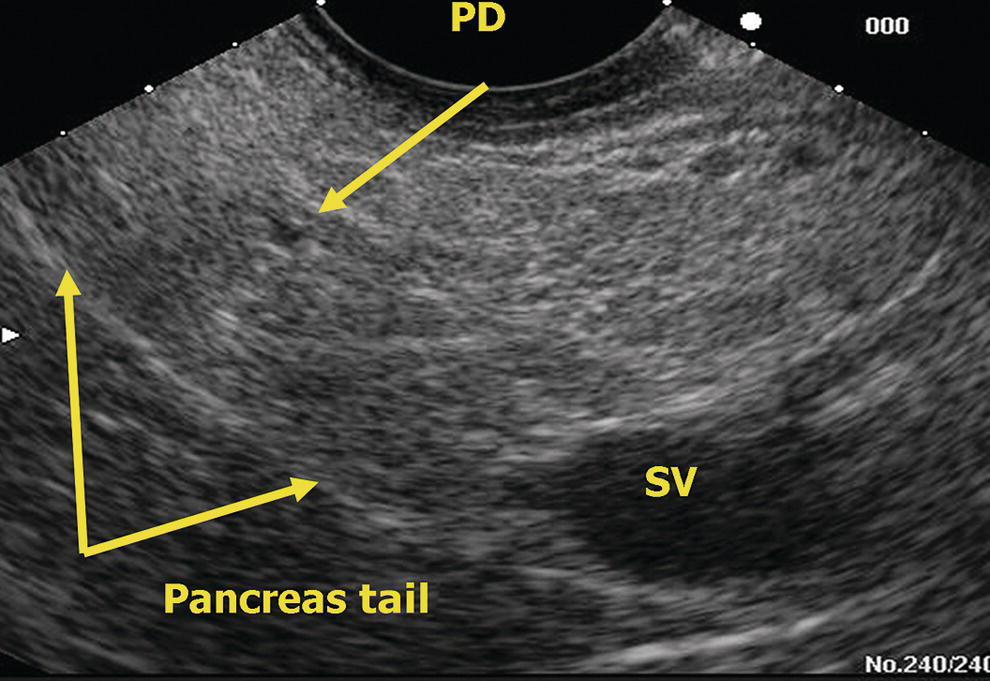
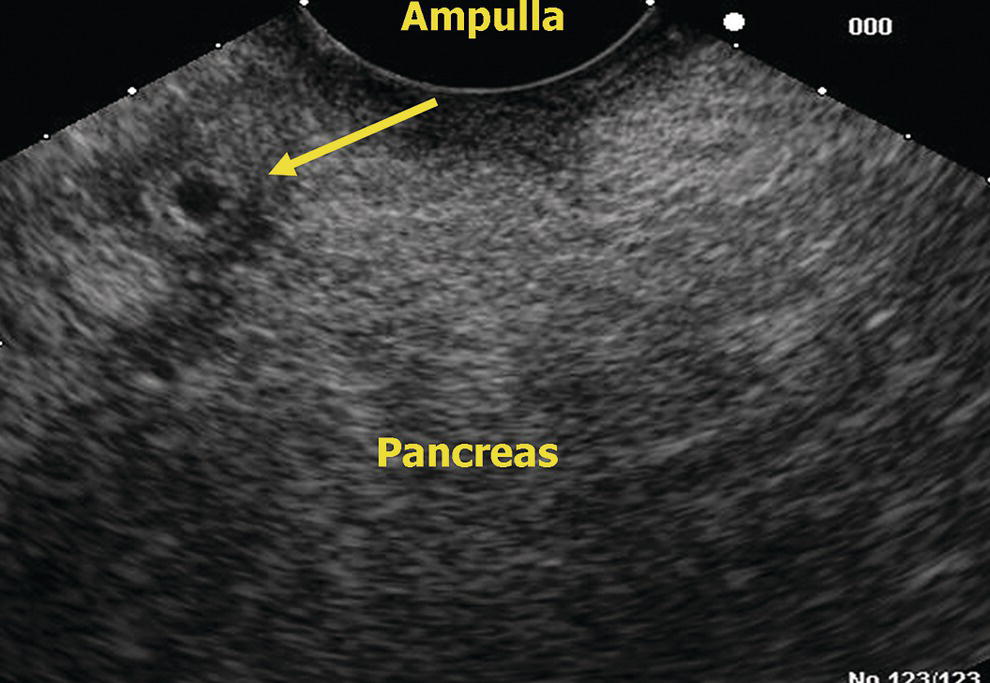
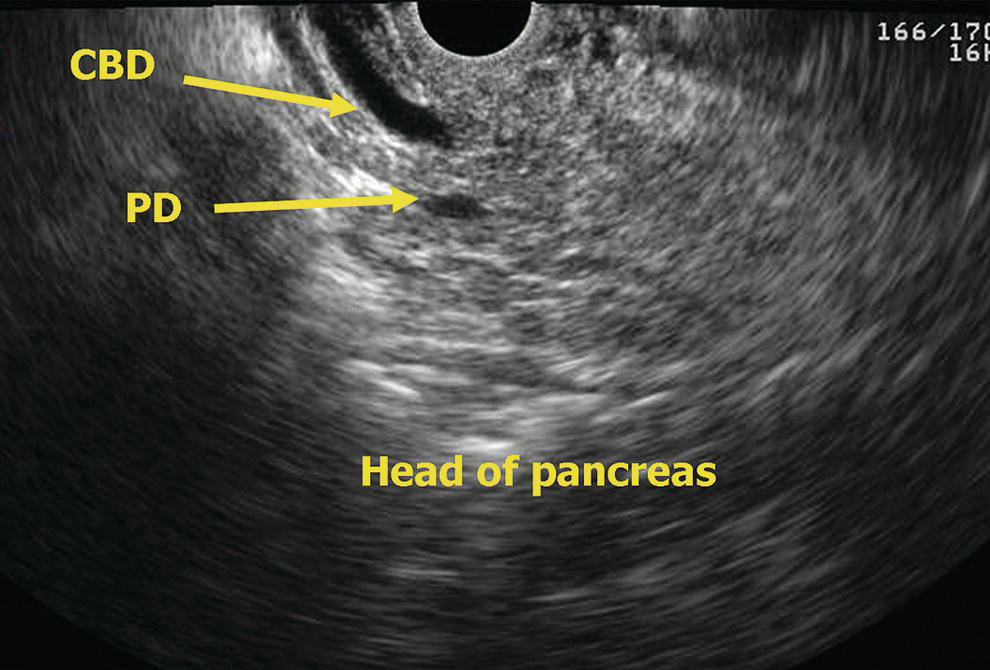
Richard A. Erickson and James T. Sing Jr. Scott and White Clinic and Hospital, and Texas A&M Health Science Center, Temple, TX, USA In radial examination of the pancreas, the organ is usually first encountered with the instrument in the mid to upper body of the stomach. On entering the stomach, the abdominal aorta can be followed a few centimeters distally to the take‐off of the celiac artery. From there, advancing the scope just a few centimeters more distally will result in it crossing the neck/body of the pancreas (Figure 6.1). The confluence of the portal vein (PV) and splenic vein (SV) should appear deep to the pancreas neck with some minor manipulations of the orientation of the echoendoscope tip. The superior mesenteric artery can be seen in cross‐section deep to the confluence surrounded by the echogenic fat of the retroperitoneum. The portal/splenic vein confluence has been described as looking like a golf club with the portal vein being the head of the club, the splenic vein the shaft, and the superior mesenteric artery the golf ball (Figure 6.2). By continuing to follow the pancreas and splenic vessels towards the patient’s left and slightly withdrawing the echoendoscope, the tail of the pancreas is imaged (Figure 6.3). Following the splenic vessels to the left will lead to the hilum of the spleen, which is an important landmark as it marks the leftward limit of the tail of the pancreas. It is important to not forget that the tail of the pancreas may move deep from the stomach wall nestled between the left kidney and spleen (Figure 6.4). If this area is not examined carefully, pancreatic tail lesions can be easily missed. From the confluence of the portal/splenic vein, gently advancing the tip of the echoendoscope forward and angulating the tip of the echoendoscope posterior one can view the pancreatic neck (Figure 6.5). Again, if this area is not examined carefully, pancreatic neck lesions may go unnoticed. On advancing the echoendoscope deep into the duodenum, the side‐by‐side cross‐sections of the inferior vena cava and abdominal aorta come into view. On withdrawing the echoendoscope from the deep duodenum, the most caudad portion of the ventral pancreas will usually come into view just to the patient’s left (counterclockwise) of the abdominal aorta (Figure 6.6). On gentle withdrawal, the ampulla can usually be located by identifying the first visible portions of pancreatic duct in the ventral pancreas (VP) and following the course of the duct by slow withdrawal towards the duodenal wall and ampulla (Figure 6.7). The triangular‐shaped ventral pancreas may appear more echolucent than the dorsal pancreas (DP) in about 75% of normal people and should not be mistaken for an echolucent tumor (Figure 6.6). The echolucency of the ventral pancreas can occasionally even be seen in views of the organ through the stomach. Further withdrawal reveals more of the pancreatic head where longitudinal views of the pancreatic duct may occasionally be seen (Figure 6.8). The confluence of the superior mesenteric vein with the portal vein and splenic vein is seen deep to the pancreatic head (Figure 6.9). This is an important view for examining splanchnic venous involvement by pancreatic head malignancies. As the echoendoscope comes around the junction of the second and first portion of the duodenum, small changes in orientation of the tip will result in major shifts in views. Sometimes the best views of the head of the pancreas are obtained when the echoendoscope first enters into the duodenal bulb with the scope in a long position. It is this orientation which most commonly provides a “stack sign” of the common bile duct (CBD) running parallel to the deeper main pancreatic duct (Figure 6.10). A stack sign can be demonstrated in more than 80% of patients with normal pancreatic ductal anatomy. When pancreas divisum exists (3–7% of normal people), a stack sign can only be demonstrated in about one‐third of patients. Instead of the absence of a stack sign in pancreas divisum the more specific crossed duct sign may be seen. The crossed duct sign results from the CBD being seen in cross‐section while the pancreatic duct, draining to the minor ampulla, is seen in longitudinal section. Figure 6.1 Radial EUS: pancreatic body and portal/splenic vein confluence. PV, portal vein; SMA, superior mesenteric artery; SV, splenic vein. Figure 6.2 Radial EUS: portal/splenic vein confluence. PV, portal vein; SMA, superior mesenteric artery; SV, splenic vein. The linear endosonographic examination of the pancreas through the stomach differs fundamentally from the radial examination in that complete imaging of the pancreas must be provided by rotating the shaft of the scope. Since the retroperitoneal structures are all posterior to the stomach, clockwise (rightward) rotation of the echoendoscope will point the echoendoscope towards the patient’s left and counterclockwise (leftward) rotation towards their right side. To find the pancreas in the stomach, one starts at the abdominal aorta near the gastroesophageal junction and follows its course distally until the take‐off of the celiac artery is visible. Usually, the more oblique take‐off of the superior mesenteric artery is apparent just distal to this. Further advancement of the instrument distally will find the pancreas neck/body nestled between the “V” of the celiac and superior mesenteric artery. The splenic artery will course tortuously in and out of the pancreas body/tail, but the splenic vein usually has a straight course and is the larger, deeper and more ovoid of the two vessels (Figure 6.11). The pancreas is interrogated sequentially from the neck to the body and tail through the stomach at this level by rotating the echoendoscope to the right (clockwise) with slight withdrawal following the splenic vein and splenic artery as they run into the hilum of the spleen. The pancreas neck, body, and tail will appear be the tissue found between the splenic vein and the posterior gastric wall. The pancreatic duct is usually seen in cross‐section through the stomach (Figure 6.12). A normal caliber duct will appear as a small, sometimes difficult to see, echolucent dot in the middle of the pancreatic parenchyma. Rotation to the left at the level of the celiac axis and body of the pancreas brings into view the pancreatic neck with the portal vein confluence deep to it. The splenic vein merges into the confluence from the patient’s left and the superior mesenteric vein runs caudad from the portal vein confluence. A little further leftward rotation of the echoendoscope may produce views of the right border of the pancreatic neck looking down towards the pancreatic head. Sometimes, longitudinal views of the pancreatic duct can be obtained from this view. Figure 6.3 Radial EUS: pancreas tail. PD, pancreatic duct; SA, splenic artery; SV, splenic vein. Figure 6.4 Radial EUS: pancreas tail. Figure 6.5 Radial EUS: pancreas neck. PD, pancreatic duct; PV, portal vein; SV, splenic vein. Figure 6.6 Radial EUS: head of pancreas. DP, dorsal pancreas; VP, ventral pancreas. Figure 6.7 Radial EUS: ampulla. Figure 6.8 Radial EUS: head of pancreas. CBD, common bile duct; PD, pancreatic duct. Figure 6.9 Radial EUS: head of pancreas, vasculature. CBD, common bile duct; PD, pancreatic duct; PV, portal vein; SMV, superior mesenteric vein; SV, splenic vein. Figure 6.10 Radial EUS: head of pancreas. CBD, common bile duct; PD, pancreatic duct. Figure 6.11 Linear EUS: pancreas body. PD, pancreatic duct; SA, splenic artery; SV, splenic vein. Figure 6.12 Linear EUS: pancreas tail. PD, pancreatic duct; SV, splenic vein. As with radial endosonography, the linear duodenum presents the endosonographer with the most variability in endosonographic relationships of vessels, ducts, and periduodenal organs. There is a marked transition in the direction of the scope tip and therefore anatomic views between entering the duodenal bulb in a “long position,” where the scope tip is pointing cephalad and posterior, and a “short position” when withdrawing from the second portion of the duodenum, where the scope tip is pointing caudad. Generally, we try to start by inserting the linear echoendoscope deep into the second portion of the duodenum. With the echoendoscope in a short position in the second portion of the duodenum, the scope is designed to be facing the medial wall of the duodenum near the region of the ampulla (Figure 6.13). On slightly rotating the scope right or left with very gentle withdrawal, usually the pancreatic duct will be seen first traveling relatively perpendicularly away from the transducer. The CBD will be seen to originate from the ampulla between the duodenal lumen and the pancreatic duct (Figure 6.14). The pancreatic parenchyma seen at the level of the ampulla represents primarily the ventral pancreas. The relative echolucency of the ventral anlage commonly seen by radial endosonography may be less apparent by linear endoscopic ultrasound (EUS). At this level, if vessels are seen deep to the pancreatic head they are usually the superior mesenteric vein and artery. If one inserts the echoendoscope deeper into the third portion of the duodenum, the uncinate portion of the pancreas nestled among the vessels of the mesenteric root may be seen. Because this is a difficult view to get with a radial instrument, this view using a linear instrument is sometimes the only way in which deep uncinate tumors may be seen. From the ampullary region, further gradual withdrawal and rotation to the left (counterclockwise) will follow the course of the tubular structures of the porta hepatis. The pancreatic head will appear as the tissue between the superior mesenteric vein/portal vein and the duodenal wall. Figure 6.13 Linear EUS: ampulla. Figure 6.14 Linear EUS: head of pancreas. CBD, common bile duct; PD, pancreatic duct. There is considerable variability in the endosonographic appearance of the pancreatic parenchyma. Classically it has a homogeneous, fine, “salt and pepper” appearance with echogenicity similar to the spleen. The ventral anlage is more echolucent because of its different embryologic origin and its lesser content of echogenic fat. In the elderly, the pancreas can get more nodular with courser echogenicity. In obese patients, the pancreas becomes infiltrated with fat and can almost disappear into the retroperitoneal fat. Fortunately, any pathologic pancreatic lesions, such as dilated ducts, cysts, or neoplasms, will be easily visible in the bright background of retroperitoneal fat. Thin patients typically offer particularly detailed imaging of the pancreas.
6
EUS of the Normal Pancreas
Radial examination of the pancreas

Linear examination of the pancreas

Endosonographic appearance of the normal pancreatic parenchyma
Related posts:
 How to do EUS‐guided Radiofrequency Ablation of Pancreatic Neuroendocrine Tumors
How to do EUS‐guided Radiofrequency Ablation of Pancreatic Neuroendocrine Tumors
 Biliary Tract Pathology
Biliary Tract Pathology
 How to Inject Chemotherapeutic Agents
How to Inject Chemotherapeutic Agents
 How to do EUS‐guided Treatment of Gastric Varices
How to do EUS‐guided Treatment of Gastric Varices
 How to use ex vivo Models in Teaching Therapeutic Endoscopic Ultrasound
How to use ex vivo Models in Teaching Therapeutic Endoscopic Ultrasound
 How to Perform Endoscopic Ultrasound‐directed Transgastric Endoscopic Retrograde Cholangiopancreatography (EDGE)
How to Perform Endoscopic Ultrasound‐directed Transgastric Endoscopic Retrograde Cholangiopancreatography (EDGE)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


