The article reviews the anatomy and imaging evaluation of the sellar and parasellar regions. Both common and uncommon sellar and suprasellar masses are reviewed, focusing on a systematic approach to analysis and when appropriate, differential creation.
- •
Anatomic localization is essential in the creation of a differential diagnosis of a sellar or parasellar region mass.
- •
Dedicated magnetic resonance imaging protocols (eg, pituitary, skull base, or sinus) are important for complete characterization, and computed tomography should be considered as a complementary modality to evaluate anatomic variants, calcification, or intraosseous extension.
- •
Certain diagnoses are dependent on the imaged patient population or clinical presentation; this knowledge further facilitates the provision of a limited, expert differential.
Introduction
The sellar and parasellar regions are anatomically and pathologically complex areas. Expert knowledge of the anatomy and diseases is important to provide focused differentials and guide patient management. Inflammatory/granulomatous, infectious, neoplastic, and vascular diseases can involve these regions, arising from the pituitary gland, infundibular stalk, hypothalamus, cranial nerves, vascular structures, leptomeninges, or skull base. Abnormalities may be detected incidentally on imaging or when imaged patients present with pituitary dysfunction, vision changes, or cranial nerve III, IV, V, or VI palsies.
Anatomy
Sellar Region
The sellar region encompasses the sella turcica and the pituitary gland. The parasellar region includes the structures and spaces bordering the sella turcica, namely the cavernous sinuses, suprasellar cistern, hypothalamus, and ventral inferior third ventricle.
The sella turcica (Turkish saddle) is a concave depression in the sphenoid bone. Its ventral borders are the tuberculum sellae and anterior clinoid processes and its dorsal borders are the dorsum sellae and the posterior clinoid processes. The roof of the sella consists of a thin dural covering: the diaphragma sellae.
Within the sella turcica, the pituitary gland consists of the ventral adenohypophysis and the dorsal neurohypophysis. The adenohypophysis is formed by ascending ectodermal cells of the Rathke pouch and consists of the pars distalis, pars intermedia, and pars tuberalis. The adenohypophysis primarily secretes regulatory hormones, such as growth, adrenocorticotropic, prolactin, follicle-stimulating, luteinizing, and thyroid-stimulating hormones.
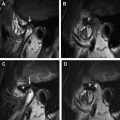
In contrast, the neurohypophysis is formed as an extension or evagination of neural ectoderm from the floor of the third ventricle (diencephalon). The neurohypophysis consists of par nervosa and infundibulum, the latter inserting into the median eminence of the hypothalamus. The infundibulum extends from the hypothalamus through the diaphragma sellae to the pituitary gland. The neurohypophysis primarily consists of axon terminals that secrete hormones formed in the hypothalamus (antidiuretic hormone [vasopressin] and oxytocin) into the blood ( Fig. 1 A, B).
Related posts:
 MR Imaging of the Temporomandibular Joint
MR Imaging of the Temporomandibular Joint
 Aggressive Inflammatory and Neoplastic Processes of the Paranasal Sinuses
Aggressive Inflammatory and Neoplastic Processes of the Paranasal Sinuses
 Applications of Magnetic Resonance Imaging in Adult Temporal Bone Disorders
Applications of Magnetic Resonance Imaging in Adult Temporal Bone Disorders
 Magnetic Resonance Imaging of the Pediatric Neck
Fetal MRI
Magnetic Resonance Imaging of the Pediatric Neck
Fetal MRI
 Patterns of Perineural Tumor Spread in Head and Neck Cancer
Patterns of Perineural Tumor Spread in Head and Neck Cancer
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


