Chapter 4
Exposure Technique Factors
After completing this chapter, the reader will be able to perform the following:
1. Define all the key terms in this chapter.
2. State all the important relationships in this chapter.
3. Explain the relationship between milliamperage and exposure time with radiation production and image receptor (IR) exposure.
4. Calculate changes in milliamperage and exposure time to change or maintain exposure to the IR.
5. Compare the effect of changes in milliamperage (mA) and exposure time on digital and film-screen images.
6. Recognize how to correct exposure factors for a density error.
7. Explain how kilovoltage peak (kVp) affects radiation production and IR exposure.
8. Calculate changes in kVp to change or maintain exposure to the IR.
9. Compare the effect of changes in kVp on digital and film-screen images.
10. Recognize the factors that affect recorded detail and distortion.
11. Calculate changes in mAs for changes in source-to-image receptor distance.
12. Calculate the magnification factor, and determine image and object size.
13. Describe the use of grids and beam restriction and their effect on IR exposure and image quality.
14. Calculate changes in mAs when adding or removing a grid.
15. Recognize patient factors that may affect IR exposure.
16. Identify the exposure factors that can affect patient radiation exposure.
17. State exposure technique modifications for the following considerations: body habitus, pediatric patients, projections and positions, soft tissue, casts and splints, and pathologic conditions.
In Chapter 2, variables that affect both the quantity and the quality of the x-ray beam were presented. Milliamperage and time affect the quantity of radiation produced, and kilovoltage affects both the quantity and the quality. Chapter 3 emphasized that a good-quality radiographic image accurately represents the anatomic area of interest. The characteristics evaluated for image quality are density or brightness, contrast, recorded detail or spatial resolution, distortion, and noise. This chapter focuses on exposure techniques and the use of accessory devices and their effect on the radiation reaching the image receptor (IR) and the image produced. Radiographers have the responsibility of selecting the combination of exposure factors to produce a good-quality image. Knowledge of how these factors affect the image individually and in combination assists the radiographer to produce a radiographic image with the amount of information desired for a diagnosis.
Primary Factors
Milliamperage and Exposure Time
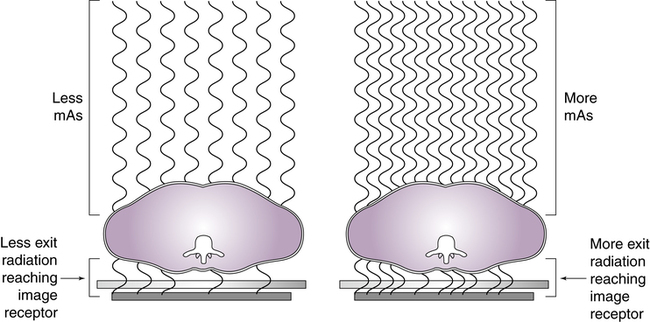
The quantity of radiation reaching the patient affects the amount of remnant radiation reaching the IR. The product of milliamperage and exposure time has a direct proportional relationship with the quantity of x-rays produced. Once the anatomic part is adequately penetrated, as the quantity of x-rays is increased, the exposure to the IR proportionally increases (Figure 4-1). Conversely, when the quantity of x-rays is decreased, the exposure to the IR decreases. Therefore, exposure to the IR can be increased or decreased by adjusting the amount of radiation (mAs).
 Important Relationship
Important Relationship Mathematical Application
Mathematical Application
Adjusting Milliamperage or Exposure Time

To increase the mAs to 40, you could use:


 Important Relationship
Important Relationship Mathematical Application
Mathematical Application


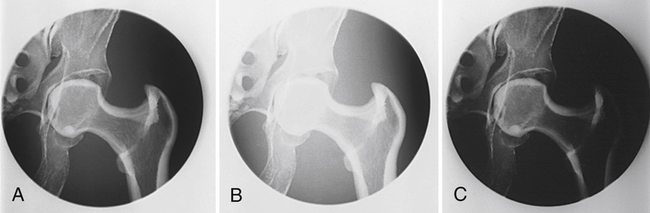
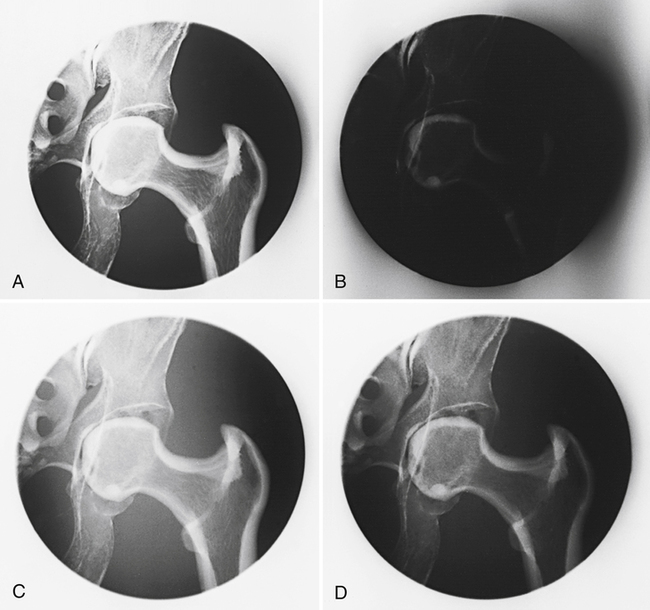
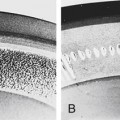
It is important for the radiographer to determine the amount of mAs needed to produce a diagnostic image. This is not an easy task because there are so many variables that can affect the amount of mAs required. For example, single-phase generators produce less radiation for the same mAs compared with a high-frequency generator. A patient’s age, the general condition of the patient, and the presence of a pathologic condition also affect the amount of mAs required for the procedure. In addition, IRs respond differently for a given mAs. Digital IRs can detect a wide range of radiation intensities (wide dynamic range) exiting the patient and are not as dependent on the mAs as film-screen IRs. However, exposure errors can adversely affect the quality of the digital image. If the mAs is too low (low exposure to the digital IR), image brightness is adjusted during computer processing to achieve the desired level. Although the level of brightness has been adjusted, there may be increased quantum noise visible within the image (Figure 4-2). If the mAs selected is too high (high exposure to the digital IR), the brightness can also adjusted, but the patient has received more radiation than necessary.
 Important Relationship
Important Relationship Important Relationship
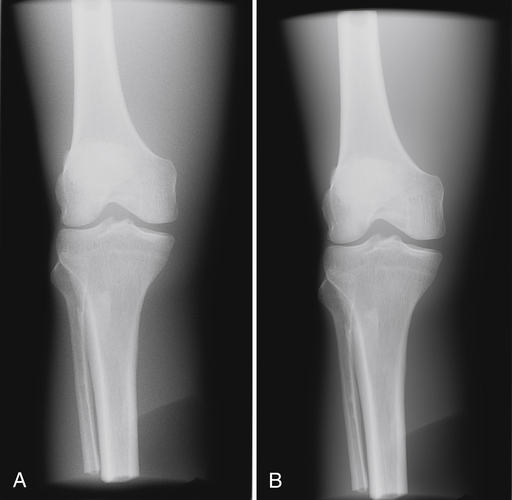
Important RelationshipFor film-screen IRs, the mAs controls the density produced in the image. There is a direct relationship between the amount of mAs and the amount of density produced when using film-screen IRs. When the mAs is increased, density is increased; when the mAs is decreased, density is decreased (Figure 4-3).
 Important Relationship
Important RelationshipKilovoltage Peak
 Important Relationship
Important RelationshipKilovoltage Peak and Exposure to the Image Receptor
 Important Relationship
Important Relationship Patient Protection Alert
Patient Protection AlertThe kVp has a greater effect on the image when using film-screen IRs. Increasing the kVp increases IR exposure and the density produced on a film image, and decreasing the kVp decreases IR exposure and the density produced on a film image (Figure 4-4).
For film-screen IRs, kVp has a direct relationship with density; however, the effect of the kVp on density is not equal throughout the range of kVp (low, middle, and high). A greater change in the kVp is needed when operating at a high kVp (>90) compared with operating at a low kVp (<70) (Figure 4-5).
 Important Relationship
Important Relationship Important Relationship
Important Relationship Mathematical Application
Mathematical Application
Using the 15% Rule
To increase exposure to the IR, multiply the kVp by 1.15 (original kVp + 15%):

To decrease exposure to the IR, multiply the kVp by 0.85 (original kVp − 15%):

To maintain exposure to the IR, when increasing the kVp by 15% (kVp × 1.15), divide the original mAs by 2:

When decreasing the kVp by 15% (kVp × 0.85), multiply the mAs by 2:

 Patient Protection Alert
Patient Protection AlertKilovoltage Peak and Radiographic Contrast
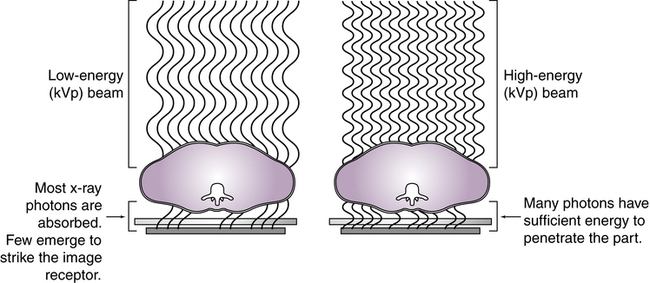
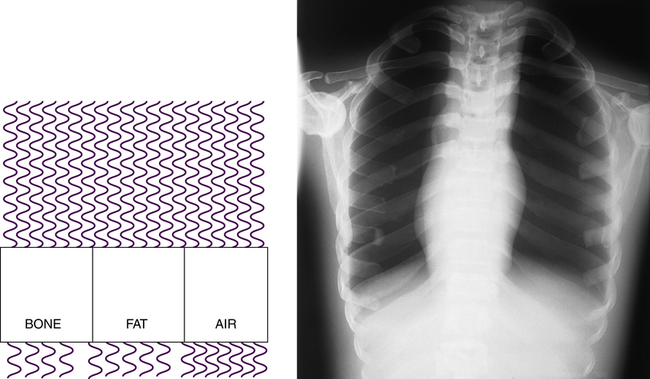
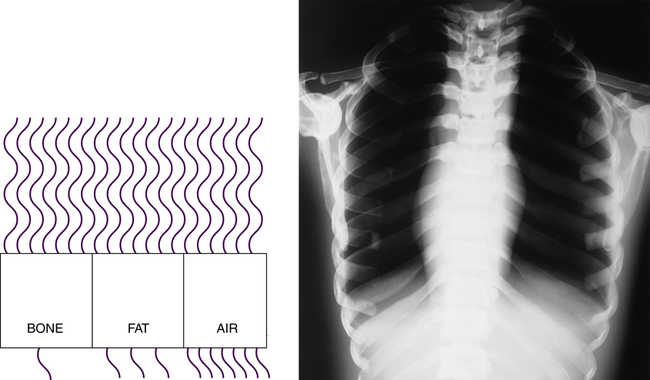
Altering the penetrating power of the x-ray beam affects its absorption and transmission through the anatomic tissue being radiographed. Higher kVp increases the penetrating power of the x-ray beam and results in less absorption and more transmission in the anatomic tissues, which results in less variation in the x-ray intensities exiting the patient (lower subject contrast). As a result, images with lower contrast (more shades of gray) are produced (Figure 4-6). When a low kVp is used, the x-ray beam penetration is decreased, resulting in more absorption and less transmission, which results in greater variation in the x-ray intensities exiting the patient (higher subject contrast). A high-contrast (fewer shades of gray) radiographic image is produced (Figure 4-7).
 Important Relationship
Important Relationship Important Relationship
Important Relationship Important Relationship
Important Relationship



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


