Chapter 8
Exposure Technique Selection
After completing this chapter, the reader will be able to perform the following:
1. Define all the key terms in this chapter.
2. State all the important relationships in this chapter.
3. State the purpose of automatic exposure control (AEC) in radiography.
4. Differentiate among the types of radiation detectors used in AEC systems.
5. Recognize how the detector size and configuration affect the response of the AEC device.
6. Explain how alignment and positioning affect the response of the AEC device.
7. Discuss patient and exposure technique factors and their effect on the response of the AEC device.
8. Analyze unacceptable images produced using AEC, and identify possible causes.
9. Recognize the effect of the type of image receptor on AEC calibration, its use, and image quality.
10. Describe patient protection issues associated with AEC.
11. State the importance of calibration of the AEC system to the type of image receptor used.
12. Define anatomically programmed radiography (APR).
13. Differentiate between the types of exposure technique charts.
Automatic Exposure Control
 Important Relationship
Important RelationshipRadiation Detectors
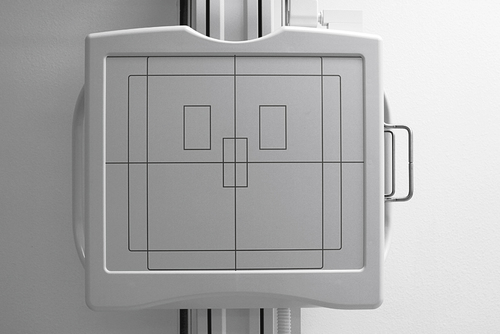
The difference in AEC systems lies in the type of device that is used to convert radiation into electricity. Two types of AEC systems have been used: phototimers and ionization chambers. Phototimers represent the first generation of AEC systems used in radiography, and it is from this type of system that the term phototiming has evolved. Phototiming specifically refers to the use of an AEC device that uses photomultiplier tubes or photodiodes, even though these systems are uncommon today. Therefore, the use of the term phototiming is usually incorrect. The more common type of AEC system uses ionization chambers. Regardless of the specific type of AEC system used, almost all systems use a set of three radiation-measuring detectors, arranged in some specific manner (Figure 8-1). The radiographer selects the configuration of these devices, determining which one (or more) of the three actually measures radiation exposure reaching the IR. These devices are variously referred to as sensors, chambers, cells, or detectors. These radiation-measuring devices are referred to here for the remainder of the discussion as detectors
 Important Relationship
Important RelationshipPhototimers
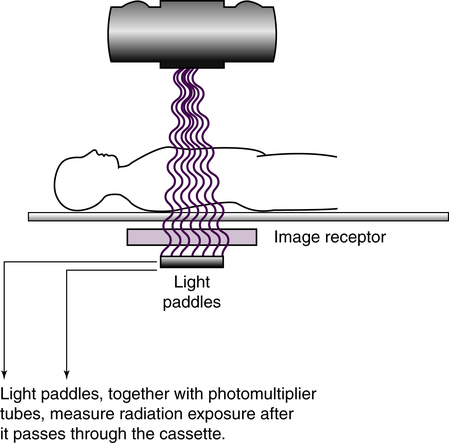
Phototimers use a fluorescent (light-producing) screen and a device that converts the light to electricity. A photomultiplier tube is an electronic device that converts visible light energy into electrical energy. A photodiode is a solid-state device that performs the same function. Phototimer AEC devices are considered exit-type devices because the detectors are positioned behind the IR (Figure 8-2) so that radiation must exit the IR before it is measured by the detectors. Light paddles, coated with a fluorescent material, serve as the detectors, and the radiation interacts with the paddles, producing visible light. This light is transmitted to remote photomultiplier tubes or photodiodes that convert this light into electricity. The timer is tripped, and the radiographic exposure is terminated when a sufficiently large charge has been received. This electrical charge is in proportion to the radiation to which the light paddles have been exposed. Phototimers have largely been replaced with ionization chamber systems.
Ionization Chamber Systems
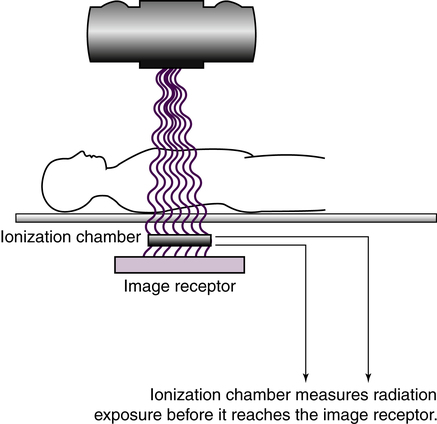
An ionization chamber, or ion chamber, is a hollow cell that contains air and is connected to the timer circuit via an electrical wire. Ionization chamber AEC devices are considered entrance-type devices because the detectors are positioned in front of the IR (Figure 8-3) so that radiation interacts with the detectors just before interacting with the IR. When the ionization chamber is exposed to radiation from a radiographic exposure, the air inside the chamber becomes ionized, creating an electrical charge. This charge travels along the wire to the timer circuit. The timer is tripped, and the radiographic exposure is terminated when a sufficiently large charge has been received. This electrical charge is in proportion to the radiation to which the ionization chamber has been exposed. Compared with phototimers, ion chambers are less sophisticated and less accurate, but they are less prone to failure. Most AEC systems today use ionization chambers.
 Important Relationship
Important Relationship Important Relationship
Important Relationship Important Relationship
Important Relationship Patient Protection Alert
Patient Protection Alert Important Relationship
Important Relationship Important Relationship
Important Relationship Important Relationship
Important Relationship Patient Protection Alert
Patient Protection AlertAlignment and Positioning Considerations
Detector Selection
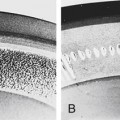
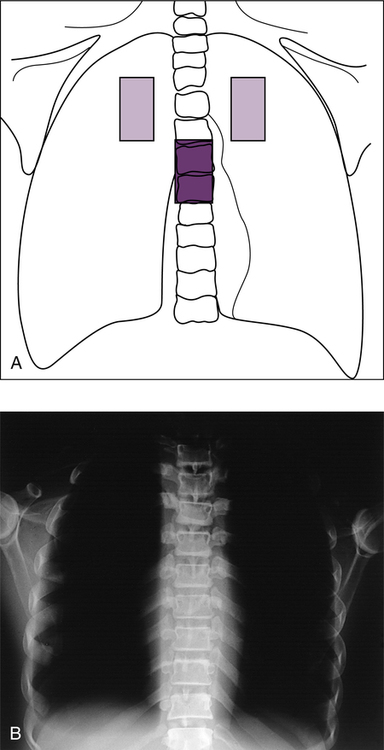
Measuring radiation that passes through the anatomic area of interest is important. The general guideline is to select the detectors that would be superimposed by the anatomic structures that are of greatest interest and need to be visualized on the radiograph. Failure to use the proper detectors could result in either underexposure or overexposure to the IR. In the case of a posteroanterior (PA) chest radiograph, the area of radiographic interest includes the lungs and heart; therefore, one or two outside detectors should be selected to place the detectors directly beneath the critical anatomic area. If the center detector were mistakenly selected, the anatomy superimposing this detector includes the thoracic spine. If the exposure is made, the resultant image shows sufficient exposure in the spine, with the lungs overexposed (Figure 8-4). In the manual that accompanies a radiographic unit, the AEC device manufacturer provides recommendations for which detectors to use for specific examinations. Recommendations for detector combination also can be found in many radiographic procedures textbooks.
 Important Relationship
Important Relationship