 FIGURE 19.1 Longitudinal ultrasound images through the midline pelvis show the normal appearances of the uterus in various developmental stages. A: Neonate with a relatively large uterus with a well-delineated endometrial stripe under the influence of maternal hormones. Notice the relative prominence of the cervix (arrowheads) with respect to the body and fundus (arrow). B: Prepubertal, tubular appearance of the uterus (arrows) in a 7-year-old girl. No endometrial stripe is seen. The uterus is homogeneously hypoechoic. C: Inverted pear-shaped appearance of the postpubertal uterus. Notice the typical appearance of the endometrial stripe in the periovulatory phase. The thin hypoechoic layer just outside of the calipers represents the inner myometrial layer and should not be included in the endometrial measurement. A small amount of free fluid (asterisk) is present in the cul-de-sac. |
conditions. When a Mullerian anomaly is known or suspected, limited imaging should be performed through the renal fossae to evaluate for renal agenesis and other anomalies. MR is also an excellent modality for evaluation of vulvar lesions when assessment of deeper structures is required.
TABLE 19.1 Normal Uterine and Ovarian Appearances During Childhood | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
uterus, cervix, and the upper two-thirds of the vagina develop. The lower one-third of the vagina develops from the urogenital sinus, and, therefore, vaginal anomalies and anomalies of the external genitalia are not always associated with Mullerian duct anomalies.5 Uterine development can be broken down into three stages. The first is organogenesis at 5 to 6 weeks,15 failure of which results in aplasia/hypoplasia, or if unilateral, a unicornuate uterus. Fusion of the two Mullerian ducts is the second stage occurring at 7 to 9 weeks and when incomplete results in a uterus didelphys or bicornuate uterus. The third stage is septal resorption, and septate and arcuate uteri are the result of at least partial septal persistence.
anomalies, particularly in the setting of oligohydramnios. At birth, abnormalities of the perineal orifices, urethra, clitoris/penis, scrotum/labia, and palpable gonads at physical examination are indications for imaging investigation of the genitourinary tract.9 Ambiguous genitalia are found in 4% to 7% of DSD patients in infancy.8 Congenital adrenal hyperplasia is the most common DSD in 46XX girls and usually presents with ambiguous genitalia and internal female reproductive organs.8,9,14 The most common defect in congenital adrenal hyperplasia is 21-α-hydroxylase deficiency, and many of these
patients have a salt-wasting disorder that may present emergently with an adrenal crisis in the first 2 weeks of life.20 Older patients with DSD may present with delayed puberty, pelvic pain, inguinal hernia, previously unrecognized genital ambiguity, primary amenorrhea, contrasexual secondary sex characteristics, or menstruation in phenotypic males presenting as recurrent hematuria.21
 FIGURE 19.2 A: Schematic drawing of female genital tract anatomy. 1. Round ligament. 2. Uterus. 3. Uterine cavity. 4. Peritoneal surface of uterus. 5. Vesical surface of uterus (toward bladder). 6. Fundus of uterus. 7. Body of uterus. 8. Palmate folds of cervical canal. 9. Cervical canal. 10. Posterior lip of cervix. 11. Cervical os (external). 12. Isthmus of uterus. 13. Supravaginal portion of cervix. 14. Vaginal portion of cervix. 15. Anterior lip of cervix. 16. Cervix. B: Schematic representation of fallopian tube anatomy. The interstitial, isthmic, ampullary, and ostial portions are shown. |
testicular tissue in genotypic females.19 46XY gonadal dysgenesis may also result in different degrees of ovotesticular dysgenesis with ambiguous internal and external organs. Turner syndrome (45XO) is characterized by streak ovaries due to loss of germ cells after 22 weeks’ gestation, despite initially normal ovarian development. Streak ovaries containing no germ cell components can also be found in 46XX ovarian dysgenesis.31 45X/46XY mosaicism and 46XX/46XY chimerism result in ovotesticular dysgenesis because of mixed genetic signals during gonadal development.19
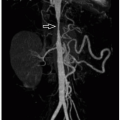
 FIGURE 19.3 A 5-year-old girl with horseshoe kidney (arrowheads). Coronal T2-weighted MR image shows that the ovaries (arrows) are abnormally high in position and located close to the midline. Left-sided pelvicaliectasis is due to ureteropelvic junction obstruction. This patient is at increased risk for a Mullerian duct anomaly given the presence of renal and urinary tract anomalies as well as maldescended ovaries. |
 FIGURE 19.4 Bicornuate bicollis uterus in a 13-year-old girl with a previously repaired cloaca malformation. A: Coronaloblique T2-weighted MR image shows two distinct, divergent uterine horns (arrows) and two distinct cervices (arrowheads). B: Coronal T2-weighted fat-saturated MR image demonstrates a malpositioned ovary with a complicated, likely hemorrhagic cyst (arrow) located well above the right iliac bifurcation. |
 FIGURE 19.5 Autopsy from a 13-year-old girl with Alstrom syndrome revealed a streak gonad (long arrow) and a hypoplastic fallopian tube (short arrow) on the left (posterior view). The right ovary (asterisk) is the expected size. |
luteinize, then regress as vascular tissue grows into the folds of the collapsed follicular walls, eventually involuting to form the corpus albicans.
 FIGURE 19.6 Neonatal ovarian cyst. A: Coronal T2-weighted fetal MR image performed at 34 weeks’ gestation shows a round, circumscribed, homogeneously hyperintense cyst (arrows) in the right abdomen. The lesion extends from the dome of the bladder (B) to the liver (L). B: Postnatal transverse gray-scale ultrasound image also shows a large simple-appearing cyst (asterisk) extending into the right upper quadrant of the abdomen. A 7 cm simple ovarian cyst was found at surgical exploration, and cystectomy was performed. The right ovary was preserved and demonstrated no evidence of torsion. RK, right kidney. |
 FIGURE 19.7 This 4.3 cm follicular cyst with luteinization (A) was excised from the ovary of a 6-year-old girl with isosexual precocity. The luteinized cells impart a yellow color to the cyst lining (B). Microscopically, the cyst lining contains follicular cells with the abundant pink and sometimes vacuolated cytoplasm that typifies “luteinized” cells (C) (hematoxylin and eosin, original magnification, 600×). |
blood flow on Doppler ultrasound evaluation and should not enhance on CT or MRI. At contrast-enhanced CT, a hemorrhagic cyst may appear hyperdense compared to other follicles, but is still less attenuating than surrounding enhanced ovarian stroma. A hematocrit effect may be observed. The MRI appearance depends upon the age of the hemorrhage. Signal hyperintensity on both non-fat-saturated and fat-saturated T1-weighted MR images is a reliable indicator of the presence of hemorrhage. These lesions may show lower than expected signal intensity on T2-weighted MR images, often referred to as “T2 shading,” which is the result of evolving blood products (Fig. 19.10). Other causes of blood-filled ovarian cysts besides corpora lutea include posttorsion/infarct and endometriotic cyst, both rare in childhood.
 FIGURE 19.8 Corpus luteum cyst, with a lumen containing a coagulum of blood (hematoxylin and eosin, original magnification, 20×). |
 FIGURE 19.9 Corpus luteum cyst becoming a hemorrhagic cyst in a 15-year-old girl. A: The corpus luteum cyst (arrow) appears as an anechoic structure with a defined wall and increased through transmission within the right ovary. B: Notice the expected low-resistance spectral Doppler waveform in the adjacent ovarian parenchyma. C: Five days later, the same cyst now contains layering echogenic debris (arrows) and low-level echoes, compatible with a hemorrhagic ovarian cyst. |
equal to 7 cm,36 although aspiration may be warranted to prevent potential torsion. Intervention may also be required for larger cysts for pain control or in case of suspected ovarian torsion, with laparoscopic cyst aspiration or cystectomy most often performed. Simple cysts larger than 7 cm require further evaluation with MR imaging or laparoscopy.36
 FIGURE 19.10 A 16-year-old girl with a hemorrhagic left ovarian cyst. A: Axial T2-weighted MR image shows a hemorrhagic cyst (arrow) in the left ovary that demonstrates “T2 shading” phenomenon due to layering blood products within the cyst. This appearance is classically associated with endometriomas, which are typically extraovarian, but can be seen in ovarian hemorrhagic cysts as well. B: Longitudinal color Doppler ultrasound image of the left ovary shows internal avascular retractile blood products within the cyst. The cyst resolved on subsequent follow-up ultrasound evaluation. (Case courtesy of Jonathan R. Dillman, MD, MSc, Cincinnati Children’s Hospital Medical Center, Cincinnati, OH.) |
 FIGURE 19.11 A 16-year-old girl with irregular menstrual cycles, severe acne, and hyperandrogenism. A: Transverse power Doppler ultrasound image of the pelvis shows bilaterally enlarged ovaries (arrowheads) containing multiple subcentimeter cysts. Ovarian volumes measure >15 mL. B: Axial T2-weighted fat-saturated MR image shows an enlarged left ovary with prominent hypointense central stroma (asterisk) and numerous peripherally arranged follicles. These findings can be seen with polycystic ovarian syndrome. Findings are more conspicuous in the left ovary due to the plane of the image. |
in these criteria. Although both ovaries are typically affected, findings may be seen in only one ovary.
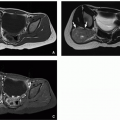
 FIGURE 19.12 A 12-year-old girl with acute pelvic pain. A: Sagittal T2-weighted MR image shows a dilated, fluid-containing right fallopian tube (arrows) with adjacent fluid. B: More lateral MR image shows an adjacent focal fluid collection associated with the right ovary (asterisk). This collection represents a tubo-ovarian abscess. C: Axial-oblique T2-weighted MR image shows the dilated fallopian tube in cross-section appearing as multiple round structures (arrows) as well as the adjacent abscess (asterisk). (Case courtesy of Jonathan R. Dillman, MD, MSc, Cincinnati Children’s Hospital Medical Center, Cincinnati, OH.) |
although 5% of simple ovarian cysts over 6 cm in children may contain malignant cells.7,48 Ovarian lesions over 8 cm are suspicious for malignancy in children.48
 FIGURE 19.13 A 17-year-old girl presented with a right-sided pyosalpinx. Transverse ultrasound (A) and coronal T2-weighted fat-saturated MR (B) images through the right lower quadrant show a dilated fallopian tube (arrows) and adjacent inflammation due to pelvic inflammatory disease. |
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


