40 Femoral Nerve Block
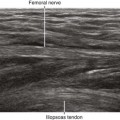
The normal femoral nerve is oval or triangular in cross section, with dimensions of about 3 mm in anteroposterior diameter and 10 mm in mediolateral diameter in the inguinal region.1 The femoral nerve usually lies lateral to the femoral artery but can contact or lie underneath the femoral artery in 15% of cases. In about one third of individuals, the femoral nerve is triangular in the suprainguinal region on short-axis scans.
The femoral nerve is covered by echogenic subcutaneous tissue and fascia. The nerve lies on the hypoechoic iliopsoas muscle, which has a characteristic mediolateral inclination. This incline positions the lateral side of the nerve slightly closer to the skin surface. At this interface of bright fascia and dark muscle, the nerve can be difficult to visualize. The best nerve visibility is proximal to the inguinal crease before the femoral nerve and femoral artery divide into smaller branches distally. In this proximal location, the femoral nerve puts a small dent in the surface of the iliopsoas muscle. This occurs because the femoral nerve usually lies in the groove between the iliacus (lateral) and psoas (medial) components of the muscle. The tilt of the transducer strongly influences femoral nerve visibility owing to anisotropic effects.2 With ultrasound guidance it may be possible to perform more proximal drug injections and therefore more complete resultant femoral nerve blocks.
Suggested Technique
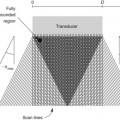
Femoral nerve block is performed in the supine position with the nerve in short-axis view. The lateral corner of the nerve is targeted to avoid the femoral vessels and to make the injection closest to the skin surface. Both out-of-plane (from distal to proximal) and in-plane (from lateral to medial) approaches can be used. It is critical that the needle tip be positioned between the fascia iliaca and iliopsoas muscle.3 It is not important to position the needle tip immediately adjacent to the nerve.
Posterior acoustic enhancement occurs deep to the femoral artery.4 This artifact should not be confused with the femoral nerve. The femoral nerve and iliopsoas tendon can be distinguished because the iliopsoas tendon normally lies deep within the iliopsoas muscle.
Many institutions have found the out-of-plane approach to be very safe and effective.5 However, the operator must be cognizant of the unimaged needle path. Branches of the femoral artery may lie within the unimaged needle path short of the scan plane.6 Scanning before needle placement can be advantageous.
The incidence of vascular puncture rates with nerve stimulation–guided femoral nerve catheters is about 6%.7 Ultrasound guidance likely reduces that incidence. Puncture of the inguinal vessels can result in blood tracking into the retroperitoneum, even if the puncture occurs distal to the inguinal ligament.8
Key Points
| Femoral Nerve Block | The Essentials |
|---|---|
| Anatomy | The FN lies lateral to the FA on the surface of the iliopsoas muscle. |
| The FN lies in the groove between the iliacus and psoas muscles. | |
| The LCFA can lie over the FN. | |
| The FN is about 3 by 10 mm in diameter. | |
| Image orientation | The iliopsoas muscle has an inclined surface from lateral to medial. |