33 Musculocutaneous Nerve Block
The musculocutaneous nerve usually passes through the coracobrachialis muscle. The musculocutaneous nerve exits the coracobrachialis between its two parts and the short head of the biceps, forming a triangle with these three muscular components.1 The musculocutaneous nerve lies between the biceps and the brachialis more distally.
Suggested Technique
Ultrasound imaging of the musculocutaneous nerve in the axilla can be used to facilitate regional block.2 This directly addresses one of the primary weaknesses of traditional axillary block.
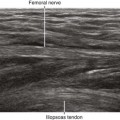
The lateral course of the nerve and its changes in shape as it passes through the coracobrachialis muscle are characteristic features that allow ultrasound identification of the nerve.3 The nerve typically has a flat shape within the coracobrachialis muscle; therefore, this is a desirable location for regional block. The relatively high surface area–to–volume ratio may improve onset kinetics of the block.
The lateral cutaneous branch of the musculocutaneous nerve can be more selectively blocked distal to the nerve exit from the coracobrachialis muscle. The point of exit is usually easy to identify because the nerve has a triangular shape in that location. Blockade of the more proximal motor fibers of the musculocutaneous nerve is unlikely with this approach. However, the nerve to the biceps brachii continues for about 4 cm after the exit from the coracobrachialis before branching off.4
The estimated incidence of pass-over musculocutaneous nerve (musculocutaneous nerve path over the coracobrachialis muscle rather than through it) ranges from 8% to 30%.5 This usually does not present a problem because the nerve can be directly imaged.
Fusion of the median nerve and musculocutaneous nerve is another common anomaly (a low-lying lateral cord). In these fusion products, the median contribution is typically larger and more superficial than the musculocutaneous contribution.6 Small muscular branches can sometimes be identified that course medial to lateral from the musculocutaneous contribution.
Key Points
| Musculocutaneous Nerve Block | The Essentials |
|---|