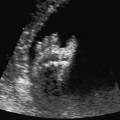
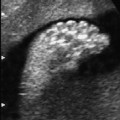
Definition: Generalized accumulation of fluid in serous body cavities, such as the pleural, peritoneal, and pericardial spaces, as well as in fetal soft tissue (skin edema), which is not caused by rhesus incompatibility. In some reports, isolated fetal ascites has also been included in this definition. Incidence: One in 2500–3500 live births. Clinical history/genetics: Many different causes are known to be responsible for this condition, so that its occurrence may be sporadic or it may be associated with certain syndromes with a variable risk of recurrence. If no cause is found, then the risk of recurrence is empirically estimated at 5%. Origin: The following disorders may cause fetal hydrops: cardiac insufficiency heads the list (anomalies, arrhythmia, volume overload due to AV anastomosis), followed by anemias (parvovirus B19, thalassemia), anomalies leading to decreased venous return to the heart (mediastinum shift due to diaphragmatic hernia or CCAM), as well as hypoproteinemia (infections, reduced protein synthesis in the liver, congenital nephrotic syndrome). Associated syndromes and causative factors: Cystic hygroma colli, cardiac anomaly (25%), arrhythmias with bradycardia and tachycardia, fetal tumors (especially coccygeal tumor, tumors within the thoracic cavity, liver tumors), lymphangiomas, malformation of the lungs (CCAM), chorioangioma of the placenta, fetal infections such as cytomegalovirus, parvovirus B19, syphilis, toxoplasmosis, varicella. Chromosomal aberrations (15%) especially Down syndrome, other trisomies, and Turner syndrome. In twin pregnancy, twin-to-twin transfusion syndrome. Others include: fetomaternal bleeding, arteriovenous shunts, obstruction of the gastrointestinal tract. Rare syndromes: achondrogenesis, α-thalassemia, Fryns syndrome, disorder of glycogen metabolism, multiple pterygium syndrome, Neu–Laxova syndrome, Noonan syndrome. Ultrasound findings: At least three of the following four findings should be detected: fetal ascites, pleural effusion, pericardial effusion, and skin edema. Pericardial effusion is often the first sign of a developing hydrops. Accompanying hydramnios is a common feature. The placenta may be swollen and thickened. Clinical management: Further ultrasound screening, including fetal echocardiography. Examination of the mother: basic blood count, hemoglobin electrophoresis, Kleinhauer–Bethke test, infection serology (TORCH), including syphilis diagnosis. Fetal examination: fetal blood sampling (umbilical venous sampling) for determination of karyotype, blood count, possibly hemoglobin electrophoresis, serum albumin, IgM, infection serology (TORCH); other parameters may be necessary using polymerase chain reaction (PCR) and virus culture from amniotic fluid. Regular ultrasound examination is mandatory. Anemia (parvovirus B19) and tachycardia can be successfully treated. In cases of pulmonary disorder (CCAM), placement of a shunt has been promising in resolving fetal hydrops in isolated cases. Hydrops due to idiopathic causes has a high rate of fetal mortality. There is a high risk of fetal distress during labor, so that primary cesarean section is a preferred clinical option if maximum intensive care is to be given to the neonate. Aspiration of ascites or pleural effusion in the prenatal stage facilitates the primary care after birth. Procedure after birth: Intensive care of the new born is needed, as they are usually severely distressed. Further treatment options depend on the cause of the hydrops. Prognosis: This depends on the cause of hydrops. A fetal mortality rate of 50–90% has been reported. References
12 Fetal Hydrops
Nonimmune Hydrops Fetalis (NIHF)
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


