Location: Most are deep tumors. Anywhere where fibrous tissue is found. Thigh, knee, trunk, arm, forearm. Rare in the head and neck. Hand and foot are most frequent sites of fibrosarcoma in the child.
Clinical: Palpable, globose, well-defined mass rarely >10 cm. It is slow growing (few weeks to 20 years). It is nearly or totally painless except when it compresses a nerve. In advanced forms it may adhere to the bone and ulcerate the skin.
Imaging: On X-rays: a mass denser than muscles. Calcifications are exceptional. Bone may be eroded or saucerized with minimal periosteal reaction. On CT: homogeneous density, compact soft tissue mass with ill-defined margins and poor enhancement after contrast administration. On MRI: inhomogeneous, lower or isointense signal as those of muscle on T1, 90 % marked, peripheral enhancement on gadolinium, and dark areas on a background of intermediate or high intensity on T2.
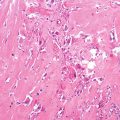
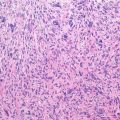
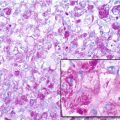
Histopathology: Low-grade well-differentiated tumor: firm, scar-like consistency, white yellow, rounded limits, growing in an expansile fashion with a pseudocapsule of reactive tissue that sharply delimits it from surrounding normal tissues. High-grade poorly differentiated tumor: soft, fish-flesh consistency, gray-white, irregular margins, growing in an invasive fashion without a capsule and with multiple processes that infiltrate the surrounding tissues, and satellites nodules isolated from the main tumor mass. On low-power view a uniform aspect of interlacing bundles of monomorphic spindle cells with interwoven parallel arranged eosinophilic collagen fibers. The cells are characteristically arranged in long, sweeping fascicles in a herringbone pattern. The cells have tapered darkly stained nuclei. High-grade lesions with marked anaplasia and pleomorphism are better classified as undifferentiated pleomorphic sarcoma. Immunohistochemistry is consistently positive for vimentin and may be positive for pan-muscle actin and smooth muscle actin.
Course and Staging: Fibrosarcoma can come from transformation of preexisting benign processes (neurofibromatosis, burn scars) and from radiation exposure. Any stage: more frequently stage IA and stage IIB. Low-grade and age <10 years are favorable prognostic factors. In children metastases are rare (<10 %). Lymph node metastases are rare (<5 %).
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


