First Trimester Pregnancy
QUESTIONS
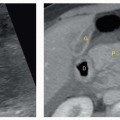
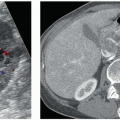
1a A 37-year-old woman presents to the ED with hyperemesis, vaginal passage of vesicles, and bloating. Laboratory work shows WBC count of 7,500. A transvaginal ultrasound shows the following:
|

Based on the history and images, what is the most appropriate next step in the management of this patient?
A. Recommend CT scan for staging as patient most likely has endometrial carcinoma.
B. Treat patient for pelvic inflammatory disease.
C. Recommend hysteroscopy and tissue sampling to exclude malignancy.
D. Ask for serum beta hCG level as findings are concerning for molar pregnancy.
View Answer
1a Answer D. The first image shows an enlarged uterus with an endometrial mass. The mass is solid with multiple small cystic spaces, the so-called “snowstorm” appearance. The next two images show bilateral enlarged ovaries, each measuring over 7 cm and containing theca lutein cysts. The findings of a solid/cystic endometrial mass with bilateral enlarged cystic ovaries is most consistent with a molar pregnancy with bilateral theca lutein cysts in a patient with this history. The beta hCG level in these patients is abnormally high, usually >100,000 mIU/mL. Theca lutein cysts occur in approximately 15% to 30% of cases of molar pregnancy because of high hCG levels. This is a case of a complete hydatidiform mole, which is the most common form of gestational trophoblastic disease. Clinical presentation includes hyperemesis gravidarum, vaginal bleeding, and vaginal passage of vesicles corresponding to hydropic villi. The uterus is typically large for dates. The conceptus is diploid with the most common karyotype being 46, XX because of fertilization of an egg devoid of genetic material by two haploid sperms with all genetic material being paternal in origin (“daddy’s little girl”).
Choices A and C are incorrect because of the history—one would not expect a woman with endometrial cancer to present with emesis, nor would she pass vesicles. Also, the 37 year old is younger than the typical patient with endometrial cancer, who is typically postmenopausal. The patient has a normal WBC count, so B is not correct.
1b This patient is at increased risk for which of the following?
A. Endometrial carcinoma
B. Hypercoagulable state
C. Persistent trophoplastic neoplasia
D. Intractable ascites
View Answer
1b Answer C. Persistent trophoblastic neoplasia (PTN) can occur after molar pregnancy—complete or partial, normal pregnancy, abortion, or ectopic pregnancy. The most common form of PTN is invasive mole characterized by trophoblastic tissue invading the myometrium. Other less common forms include choriocarcinoma, which is prone to distant metastases, and placental site trophoblastic neoplasia, which is the most lethal and rare form of PTN.
Reference: Hertzberg BS, Middleton WD. Ultrasound: the requisites, 3rd ed. Philadelphia, PA: Elsevier, 2016:349-352.
2a A 29 years old hemodynamically stable female presents with right pelvic pain. Serum beta hCG is 3,520 mIU/mL. Images from transvaginal pelvic ultrasound are shown.
|

Based on the Society of Radiologists in Ultrasound (SRU) Multispecialty Consensus Conference on “Early first trimester diagnosis of Miscarriage and Exclusion of a Viable Intrauterine pregnancy” published in October 2012, which of the following is the most appropriate next step?
A. Imaging findings are diagnostic of pregnancy of unknown location. The patient should be referred for the management of presumed ectopic pregnancy by IM methotrexate or other pharmacologic or surgical methods.
B. A viable intrauterine pregnancy is likely; serial beta hCG measurements and pelvic sonography should be performed.
C. A viable intrauterine pregnancy is possible but unlikely; however, at least one follow-up hCG measurement and follow-up pelvic US should be performed before treatment for ectopic pregnancy.
D. Findings are diagnostic of failed intrauterine pregnancy. The patient should be referred for dilatation and curettage.
View Answer
2a Answer C. Pelvic US images show normal uterus and normal bilateral ovaries. No intrauterine gestational sac or fluid is shown. No abnormal adnexal masses are shown either.
As per recommendations of the Society of Radiologists in Ultrasound (SRU) Multispecialty Consensus Conference on “Early first trimester diagnosis of Miscarriage and Exclusion of a Viable Intrauterine pregnancy” published in October 2012, if a single hCG measurement is ≥3,000 mIU/mL, a viable intrauterine pregnancy is possible but unlikely. However, the most likely diagnosis is a nonviable intrauterine pregnancy, so it is generally appropriate to get at least one follow-up hCG measurement and follow-up ultrasonogram before undertaking treatment for ectopic pregnancy.
2b Additional images of the right adnexa are shown.
|

The positive predictive value (PPV) of the findings shown in establishing the diagnosis of ectopic pregnancy is:
A. 75%
B. 85%
C. 95%
D. 100%
View Answer
2b Answer D. Images of the right adnexa show a living embryo with cardiac activity. In patients with positive pregnancy test and no evidence of intrauterine pregnancy (IUP), the positive predictive value (PPV) of this finding is 100% in diagnosing an ectopic pregnancy. The PPV of an adnexal mass containing either a yolk sac or nonliving embryo also approaches 100%. A “Tubal” or “adnexal” ring surrounding a fluid collection has PPV of 95% and a complex or solid adnexal mass without embryo, yolk sac, or tubal ring has PPV of 92%.
References: Doubilet PM, Benson CB, Bourne T, et al. Diagnostic criteria for nonviable pregnancy early in the first trimester. Ultrasound Q 2014;30(1):3-9.
Hertzberg BS, Middleton WD. Ultrasound: the requisites, 3rd ed. Philadelphia, PA: Elsevier, 2016:333-343.
3 What is the earliest intragestational sac structure to be visualized at ultrasound that can absolutely confirm an intrauterine pregnancy?
A. Amnion
B. Embryo
C. Yolk sac
D. Placenta
View Answer
3 Answer C. The yolk sac is the primary maternal-fetal transport system before a functioning placental circulation has fully developed. It is a round 3 to 5 mm cystic structure, found eccentrically located within the gestational sac, and resides within the chorionic cavity. The yolk sac can be visualized by approximately 5.5 weeks of gestational age.
 Transvaginal US image of the uterus shows the yolk sac (yellow arrow). |
By approximately 6 weeks of gestational age, the embryo can be identified as a 1 to 2 mm echogenic focus along the periphery of the yolk sac. It resides within the amniotic cavity.
The amniotic membrane is thinner than the yolk sac and is seen more easily after 7 weeks but can be seen as early as 6.5 weeks of gestational age. The amnion and chorion fuse at 14 to 16 weeks.
 Transvaginal US image of the uterus shows the amnion (red arrow) and the embryo (white arrow). |
References: Bree R, Edwards M, Bohm-Velez M, et al. Transvaginal sonography in the evaluation of normal early pregnancy: correlation with HCG level. AJR Am J Roentgenol 1989;153(1):75-79.
Lindsay DJ, Lovett IS, Lyons EA, et al. Yolk sac diameter and shape at endovaginal US: predictors of pregnancy outcome in the first trimester. Radiology 1992;183(1):115-118.
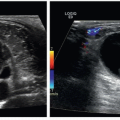
4 A 31-year-old woman presents to the emergency department with persistent vaginal bleeding after undergoing medical termination of pregnancy 4 weeks ago. Laboratory values are as follows: WBC 7,418, Hgb 6.1, Hct 19.1, beta-hCG 2,717. What is the most likely diagnosis?
|

A. Endometrial hematoma
B. Uterine arteriovenous malformation
C. Retained products of conception
D. Endometritis
View Answer
4 Answer C. The first image shows an abnormally thickened endometrium containing a solid mass with cystic spaces. The second image shows Doppler flow within the mass. Based on the images provided, the clinical history, and laboratory values, the correct answer choice is C, that is, retained products of conception. Women with retained products of conception (RPOC) typically present with abnormal bleeding and is most common after second trimester spontaneous abortion, extreme preterm birth, medical termination of pregnancy, and placenta accreta. The diagnosis is suggested when there is a mass in the endometrial canal that shows Doppler flow. However, lack of flow does not exclude RPOC. Calcifications in the mass, because of normal placental maturation, are highly suggestive of RPOC.
Choice A, endometrial hematoma, is not the correct answer because there is Doppler flow in the mass, which would not be present in a hematoma. Choice B, uterine arteriovenous malformation (AVM), can occur in the post abortion and postpartum periods with severe vaginal bleeding. Sonographically, they can present as multiple serpiginous structures within the myometrium, or as a myometrial or endometrial mass. However, these lesions are rare, and the beta hCG level should not be elevated as it is in this case. Choice D, endometritis, may show endometrial thickening and may or may not contain fluid and gas. However, clinically these patients present with fever and an elevated WBC count. This patient’s WBC count is normal.
Reference: Rumack CM, Wilson SR, Charboneau WJ. Diagnostic ultrasound, 4th ed. Philadelphia, PA: Elsevier Health Sciences, 2011:560-561, 1521-1523.

A. Monochorionic, monoamniotic
B. Monochorionic, diamniotic
C. Dichorionic, monoamniotic
D. Dichorionic, diamniotic
View Answer
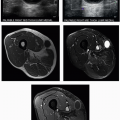
5 Answer D. This is an example of a dichorionic, diamniotic pregnancy. A thick membrane separates the two fetuses. A thin membrane is what separates monochorionic, diamniotic twin pregnancies and is usually barely perceptible on ultrasound. Also, this image is a good example of the “twin peak” or “lambda” sign, where a triangular-shaped portion of the chorion extends between the two chorionic sacs. This sign helps to confirm the presence of two chorions. Once two chorions have been established, the pregnancy must be dichorionic, diamniotic as dichorionic, monoamniotic twin pregnancies do not exist.
Reference: Hertzberg BS, Middleton WD. Ultrasound: the requisites, 3rd ed. Philadelphia, PA: Elsevier, 2016:496-497.
6 In the setting of a positive pregnancy test, the presence of an intrauterine fluid collection with a smooth, rounded or oval contour most likely represents which of the following?
|

A. Ectopic pregnancy
B. Intrauterine pregnancy
C. Adenomyosis
D. Spontaneous abortion
View Answer
6 Answer B. Although the presence of the intradecidual or double sac sign is highly suggestive of an intrauterine pregnancy (IUP), the absence of these signs does not exclude an IUP. Fluid secretions or blood within the uterine cavity in the setting of an ectopic pregnancy is referred to as a pseudogestational sac or decidual cast but occurs in only approximately 10% of ectopic pregnancies. The low incidence of pseudogestational sacs in addition to the much greater incidence of intrauterine pregnancies in general results in a >99.5% likelihood that a smooth, rounded, or oval intrauterine fluid collection represents a gestational sac in a pregnant patient. Therefore, these collections should be treated as IUPs until proven otherwise.
The term pregnancy of unknown location is used when ultrasound shows no definite IUP and normal adnexa. The differential diagnosis includes a very early IUP, occult ectopic pregnancy, and a completed spontaneous abortion.
References: Barnhart KT. Ectopic pregnancy. N Engl J Med 2009;361(4):379-387.
Campion EW, Doubilet PM, Benson CB, et al. Diagnostic criteria for nonviable pregnancy early in the first trimester. N Engl J Med 2013;369(15):1443-1451.
Doubilet PM, Benson CB. First, do no harm…to early pregnancies. J Ultrasound Med 2010;29(5):685-689.
Rodgers SK, Chang C, DeBardeleben JT, et al. Normal and abnormal US findings in early first-trimester pregnancy: review of the society of radiologists in ultrasound 2012 consensus panel recommendations. RadioGraphics 2015;35(7):2135-2148.
7 What is the crown rump length established by the Society of Radiologists in Ultrasound at which cardiac activity should be present?
A. 3 mm
B. 5 mm
C. 7 mm
D. 9 mm
View Answer
7 Answer C. Cardiac activity may be detected in embryos as small as 1 to 2 mm, corresponding to approximately the 6th week of gestation. However, the absence of cardiac motion may be normal in embryos smaller than 4 mm. In order to account for differing equipment types, measurement variability, and other variations in ultrasound imaging, a crown-rump length of 7 mm or greater has been established by the Society of Radiologists in Ultrasound as the size at which cardiac activity should be present. A definitive diagnosis of failed pregnancy requires that an embryo is at least 7 mm and lacks cardiac activity.
References: Campion EW, Doubilet PM, Benson CB, et al. Diagnostic criteria for nonviable pregnancy early in the first trimester. N Engl J Med 2013;369(15):1443-1451.
Rodgers SK, Chang C, DeBardeleben JT, et al. Normal and abnormal US findings in early first-trimester pregnancy: review of the society of radiologists in ultrasound 2012 consensus panel recommendations. RadioGraphics 2015;35(7):2135-2148.
8 An anechoic round structure within the head at 8 to 10 weeks of gestation most likely represents which of the following?
|

A. Normal ventricles
B. Ventriculomegaly
C. Rhombencephalon
D. Anencephaly
View Answer
8 Answer C. The rhombencephalon is visible on all exams at 8 to 10 weeks as an anechoic round structure within the head, representing the developing hindbrain (medulla, pons, and cerebellum).
Anencephaly is the most common anomaly affecting the central nervous system and results from failure of closure of the rostral portion of the neural tube. The important ultrasound feature is an absent cranium, which allows diagnosis from 11 weeks onward.
Mild ventriculomegaly is defined as being present when the width of the lateral ventricle, measured at the atrium, is ≥10 mm.
References: Cardoza JD, Goldstein RB, Filly RA. Exclusion of fetal ventriculomegaly with a single measurement: the width of the lateral ventricular atrium. Radiology 1988;169(3):711-714.
Cyr DR, Mack LA, Nyberg DA, et al. Fetal rhombencephalon: normal US findings. Radiology 1988;166(3):691-692.
Johnson SP, Sebire NJ, Snijders RJM, et al. Ultrasound screening for anencephaly at 10-14 weeks of gestation. Ultrasound Obstet Gynecol 1997;9(1):14-16.
Rodgers SK, Chang C, DeBardeleben JT, et al. Normal and abnormal US findings in early first-trimester pregnancy: review of the society of radiologists in ultrasound 2012 consensus panel recommendations. RadioGraphics 2015;35(7):2135-2148.
9 A 26-year-old female presents with pelvic cramping in the first trimester. The clinical significance of the abnormality shown depends on which of the following criteria?
|

A. Length of time
B. Size
C. Gestational age
D. Patient’s age
View Answer




9 Answer B. The ultrasound image shows a crescentic hypoechoic fluid collection adjacent to the gestational sac in the endometrial cavity consistent with subchorionic hemorrhage.
The incidence of subchorionic hemorrhage in first trimester pregnancies with vaginal bleeding has been reported to be 18% to 22%. Large hematomas encircling more than two-thirds of the chorionic circumference are associated with doubling of the risk of pregnancy loss.
References: Bennett GL, Bromley B, Lieberman E, et al. Subchorionic hemorrhage in first-trimester pregnancies: prediction of pregnancy outcome with sonography. Radiology 1996;200(3):803-806.
Leite J, Ross P, Rossi AC, et al. Prognosis of very large first-trimester hematomas. J Ultrasound Med 2006;25(11):1441-1445.
Rodgers SK, Chang C, DeBardeleben JT, et al. Normal and abnormal US findings in early first-trimester pregnancy: review of the society of radiologists in ultrasound 2012 consensus panel recommendations. RadioGraphics 2015;35(7):2135-2148.
Related posts:


Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
