Neck
QUESTIONS
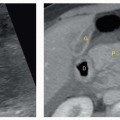
1a A 21-year-old female presents with a palpable painless lump in the anterior neck. Ultrasound images of the neck just below the level of the hyoid bone are shown. The most likely diagnosis is:
|

A. 2nd branchial cleft cyst
B. Thyroglossal duct cyst
C. Suppurative lymph node
D. Cystic nodal metastasis
View Answer
1a Answer B. Thyroglossal duct cyst (TDC) is the most common congenital neck mass. It is located in the midline (75%) or slightly off midline (25%) in the anterior neck. Most TDCs are located either at the level of (15%) or immediately below (65%) the hyoid bone. They most commonly present as a gradually enlarging painless mass in the midline of the neck in children or young adults. An uncomplicated TDC may appear as an anechoic, well-circumscribed cyst with increased through transmission or can be pseudosolid in appearance with homogenous low-level internal echoes because of the presence of proteinaceous fluid content, cholesterol crystals, and keratin. TDCs with previous infection or hemorrhage may appear as heterogeneous complex cysts with internal echoes.
The 2nd branchial cleft cyst (BCC) usually presents as a cystic neck mass posterolateral to the submandibular gland, lateral to carotid space, and anterior to sternocleidomastoid. Most 2nd BCCs are at or immediately caudal to the angle of mandible. A suppurative lymph node usually presents as a painful neck mass with skin erythema, fever, poor oral intake, and elevated white blood cell count. Cystic nodal metastases are most commonly from squamous carcinoma of the upper aerodigestive tract and papillary carcinoma of the thyroid. The nodes are often multiple and on ultrasound usually show a solid component with abnormal vascularity.
1b In which of the following situations is preoperative thyroid scintigraphy indicated in patients with thyroglossal duct cysts?
A. When a normal thyroid gland is identified by sonography
B. When a normal thyroid gland is not identified by sonography
C. When a solid vascular component is identified within the cyst
D. When a solid vascular component is not identified within the cyst
View Answer
1b Answer B. The presence of a normal thyroid gland should be confirmed during a preoperative ultrasound of a TDC because if the ectopic thyroid tissue in a TDC is the patient’s only functioning thyroid tissue, then a resection of the ectopic thyroid with the cyst will cause hypothyroidism. Preoperative identification of normal thyroid gland on ultrasound is sufficient to exclude the diagnosis of ectopic thyroid tissue and helps to avoid thyroid scintigraphy, which should be minimized, if possible, especially in pediatric patients.
The presence of a solid vascular component in a TDC should raise the suspicion of thyroglossal duct carcinoma. Fine needle aspiration (FNA) can be performed to confirm the diagnosis preoperatively. Thyroglossal duct carcinoma is an uncommon complication of TDC, occurring in <1% of cases.
References: Ahuja AT, Wong KT, King AD, et al. Imaging for thyroglossal duct cyst: the bare essentials. Clin Radiol 2005;60(2):141-148.
Hertzberg BS, Middleton WD. Ultrasound: the requisites, 3rd ed. Philadelphia, PA: Elsevier, 2016:229-230.
Kutuya N, Kurosaki Y. Sonographic assessment of thyroglossal duct cysts in children. J Ultrasound Med 2008;27(8):1211-1219.
2 Punctate echogenic foci are identified within a thyroid nodule. Identification of which of the following additional imaging features would suggest the echogenic foci are colloid as opposed to microcalcifications?
A. Posterior acoustic shadow
B. Comet-tail artifact
C. Increased through transmission
D. Refraction artifact
View Answer
2 Answer B. Comet-tail artifact is a form of reverberation artifact. Identification of a prominent (>1 mm) comet-tail artifact posterior to a linear echo within a thyroid nodule is a key imaging feature of colloid. An article by Malhi et al. showed that small (<1 mm) comet-tail artifacts may be seen posterior to echogenic foci in malignant nodules.
Acoustic shadowing is produced distal to a highly attenuating object such as a calcification. Microcalcifications in thyroid nodules are often too small to produce a posterior acoustic shadow. Increased through transmission occurs posterior to a weakly attenuating material. Whereas increased through transmission may be seen posterior to a colloid cyst, it would not be expected to be seen posterior to an echogenic focus of colloid. Refraction artifact occurs when the ultrasound beam travels through two adjacent materials with different inherent sound propagation velocities. This artifact results in misplacement of objects on the image.
References: Feldman MK, Katyal S, Blackwood MS. US artifacts. RadioGraphics 2009;29(4):1179-1189.
Frates MC, Benson CB, Charboneau JW, et al. Management of thyroid nodules detected at US: Society of Radiologists in ultrasound consensus conference statement 1. Radiology 2005;237(3):794-800.
Malhi H, Beland MD, Cen SY, et al. Echogenic foci in thyroid nodules: significance of posterior acoustic artifacts. AJR Am J Roentgenol 2014;203(6):1310-1316.
3 Identification of which of the following imaging features in a cervical lymph node would be concerning for malignancy?
A. Round shape
B. 6 mm short-axis diameter
C. Hyperechoic hilum
D. Hilar vessels
View Answer
3 Answer A. Benign or reactive cervical lymph nodes tend to have an oval shape whereas malignant lymph nodes tend to be round with a short-axis-to-long-axis ratio >0.5. There is no consensus for a cutoff short-axis diameter for cervical lymph nodes. Both malignant and reactive lymph nodes may become enlarged. An echogenic hilum that is contiguous with the surrounding perinodal fat is considered a benign appearance. An echogenic hilum may not be seen in smaller lymph nodes <5 mm. Occasionally, malignant nodes will have an echogenic hilum, so this feature should not be considered diagnostic of a benign lymph node in and of itself. Hilar vessels are expected in benign or reactive lymph nodes. Malignant lymph nodes may show peripheral vascularity.
Reference: Ying M, Bhatia KSS, Lee YP, et al. Review of ultrasonography of malignant neck nodes: greyscale, Doppler, contrast enhancement and elastography. Cancer Imaging 2013;13(4):658-669.
4 According to both the 2005 Society of Radiologists in Ultrasound (SRU) consensus statement and 2015 American Thyroid Association (ATA) guidelines, what is the next best step in management for the 1.6 cm thyroid lesion shown?
|

A. Fine needle aspiration
B. MRI for further characterization
C. PET-CT
D. No additional management required
View Answer
4 Answer D. This lesion is anechoic with posterior acoustic enhancement, which tells us that the lesion is cystic, a benign pattern. There is no solid or nodular component. According to both SRU consensus statement and 2015 ATA guidelines, fine needle aspiration is not necessary for entirely cystic lesions. MRI and PET-CT do not play a role in further characterization of thyroid nodules.
References: Frates MC, Benson CB, Charboneau JW, et al. Management of thyroid nodules detected at US: Society of Radiologists in ultrasound consensus conference statement 1. Radiology 2005;237(3):794-800.
Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016;26(1):1-133.
5a The American College of Radiology formed an Incidental Thyroid Findings Committee on managing incidental thyroid nodules (ITNs) detected on imaging in 2013. According to the guidelines published in February 2015, incidentally detected thyroid nodules on CT, MRI, and extra thyroid ultrasound (such as carotid Doppler) without suspicious features in the general population are stratified based on which two main criteria?
A. Clinical symptoms and patient sex
B. Patient age and thyroid nodule size
C. The shape and number of nodules
D. Risk stratification and nodule appearance
View Answer
5a Answer B. The American College of Radiology formed the Incidental Thyroid Findings Committee to provide guidance on managing thyroid nodules detected on medical imaging (other than dedicated thyroid ultrasound) that were previously unsuspected. The committee recommendations were published in a white paper in February 2015. The goals of the committee were to determine which incidentally detected thyroid nodules should undergo thyroid ultrasound, to reduce the costs and risks associated with follow-up ultrasound and thyroid FNA (fine needle aspiration), and to achieve consistency in reporting and managing of incidental thyroid nodules and providing guidance to radiologists who are concerned about not reporting or recommending additional workup for incidental thyroid nodules that later prove to be clinically important.
It is known that thyroid nodules are very common, found in up to 50% of patients without clinical history of thyroid disease, and majority of these nodules are multiple. Up to 25% of patients will have an incidentally detected thyroid nodule when undergoing CT and MRI studies (which include the thyroid). Malignancy rates vary based on how the nodule was detected. In large population-based studies, most incidentally detected thyroid nodules on ultrasound are found to be benign (the malignancy rate was 1.6% in patients with 1 or more nodules). On the other hand, when the nodule presents with focal uptake on 18FDG-PET scans, as many as 33% to 35% are malignant. Although autopsy studies have shown that the background rate of papillary thyroid cancer is as high as 36% of thyroid glands, most are well-differentiated small (<1 cm) papillary thyroid carcinomas with an excellent prognosis. Other studies showed that thyroid cancers <2 cm also have an indolent course, with 99.9% 10-year survival rates.
A 3-tiered system was adopted from Duke to guide the evaluation of incidentally detected thyroid nodules based on the patient’s age and imaging findings. With this system, further evaluation with thyroid ultrasound is considered for three groups: (1) nodules with certain imaging features associated with high risk (suspicious adenopathy, local invasion, and PET avidity), (2) nodules ≥1 cm in patients age <35 years, and (3) nodules ≥ to 1.5 cm in patients age ≥35 years of age. Studies have shown that the application of these criteria could decrease the rate of thyroid ultrasound recommendations by about 46% (compared to a 1-cm size cutoff) and decrease the rate of ultrasound-guided biopsies by 35%. The 3-tiered system has a 13% false-negative rate, but when including all thyroid cancers, this accounts for only 1.2% of all thyroid malignancies.
References: Hoang JK, Langer JE, Middleton WD, et al. Managing incidental thyroid nodules detected on imaging: white paper of the ACR incidental thyroid findings committee. J Am Coll Radiol 2015;12(2):143-150.
Rumack CM, Wilson SR, Charboneau WJ. Diagnostic ultrasound, 4th ed. Philadelphia, PA: Elsevier Health Sciences, 2011:712-715.
5b A 41-year-old man undergoes a chest CT pulmonary angiogram for shortness of breath where a 1.2-cm incidental hypoattenuating nodule was found confined to the right thyroid lobe. Visualized lymph nodes at the base of the neck measured <8 mm in short axis. According to the white paper on incidentally detected thyroid nodules mentioned above, what would be the most appropriate next step in management?
A. Recommend further evaluation with thyroid ultrasound.
B. Recommend further evaluation with thyroid ultrasound and ultrasound-guided biopsy.
C. Recommend referral to an endocrinologist.
D. No further evaluation is recommended.
View Answer
5b Answer D. According to the white paper on incidentally detected thyroid nodules proposed by the Incidental Thyroid Findings Committee, in patients within the general population with normal life expectancy and without suspicious imaging findings, it is the patient age and nodule size that determine the need for additional workup. Further workup with thyroid ultrasound is recommended for patients <35 years old with incidentally detected nodules measuring ≥1 cm in the axial plane. For patients age 35 or older, the size cutoff for further evaluation is raised to 1.5 cm. In this scenario, because the patient is above 35 years of age and the nodule measures under 1.5 cm, no further workup is recommended. Patients with limited life expectancy and comorbidities do not need further evaluation of incidental thyroid nodules unless it is warranted clinically or requested by the patient or referring physician. The need for nodule biopsy is based on results of the thyroid ultrasound unless the nodule is found to be 18FDG-PET avid in which case a biopsy is recommended regardless of the ultrasound appearance in patients with a normal life expectancy.
Reference: Hoang JK, Langer JE, Middleton WD, et al. Managing incidental thyroid nodules detected on imaging: white paper of the ACR incidental thyroid findings committee. J Am Coll Radiol 2015;12(2):143-150.
6a A 35-year-old otherwise healthy female was referred for ultrasound after her thyroid was noted to be diffusely enlarged on physical exam and thyroid function tests were abnormal. After reviewing her ultrasound and further questioning, she reports weight gain and constipation. The most likely diagnosis is:
|

A. Multinodular goiter
B. Graves disease
C. Radiation/radioiodine-induced hypothyroidism
D. Hashimoto thyroiditis
E. de Quervain (subacute granulomatous) thyroiditis
View Answer
6a Answer D. The ultrasound image reveals an enlarged, heterogenous thyroid lobe with innumerable small hypoechoic foci termed micronodulation very characteristic of Hashimoto thyroiditis (HT). Micronodulation is a highly sensitive sign of HT. It is caused by thyroid gland infiltration and destruction of thyroid follicles by lymphocytes and plasma cells. An associated fibrotic reaction then creates the appearance of echogenic bands in the gland in more advanced disease. Other sonographic features often present are central compartment adenopathy (usually inferior to the thyroid gland) and nodular contour of the thyroid gland. Vascularity of the thyroid is variable, but is often increased.
HT is the most common cause of hypothyroidism in the United States. The onset of hypothyroidism symptoms is often insidious including fatigue, dry skin, weight gain, and constipation. The condition, as with other causes of thyroiditis, has a strong female predominance, presenting in young to middle-aged women with painless thyromegaly. Serology usually confirms positive autoantibodies to anti-TPO (antithyroid peroxidase) and anti-Tg (antithyroglobulin).
Graves disease is an autoimmune disease of the thyroid gland also often associated with thyromegaly, parenchymal coarsening, and diffuse hypoechogenicity due to the presence of large intraparenchymal vessels and lymphocytic infiltration. Unlike in HT, the patients are hyperthyroid. The marked thyroid hypervascularity that is seen in Graves’ on color Doppler has been termed “thyroid inferno.” Micronodulation is not typical of Graves disease. Radiation-induced hypothyroidism is incorrect because the thyroid is usually small and is preceded by a history of radioiodine ablation or external beam. de Quervain thyroiditis is a type of subacute thyroiditis that typically presents with painful, hypoechoic, hypovascular lesions in the thyroid that can appear mass-like or diffuse. The condition is accompanied by hyperthyroidism at first, followed by a hypothyroid interval before returning to normal.
References: Hertzberg BS, Middleton WD. Ultrasound: the requisites, 3rd ed. Philadelphia, PA: Elsevier, 2016:237-238.
Rumack CM, Wilson SR, Charboneau WJ. Diagnostic ultrasound, 4th ed. Philadelphia, PA: Elsevier Health Sciences, 2011:741-746.
Sholosh B, Borhani AA. Thyroid ultrasound part 1: technique and diffuse disease. Radiol Clin North Am 2011;49(3):391-416.
6b Hashimoto thyroiditis is associated with an increased incidence of what type of malignancy?
A. Anaplastic thyroid carcinoma
B. Medullary thyroid carcinoma
C. Non-Hodgkin thyroid lymphoma
D. Metastatic disease to the thyroid
View Answer
6b Answer C. Primary thyroid lymphoma is a rare cause of malignancy accounting for <5% of thyroid malignancies. Most thyroid lymphomas are non-Hodgkin lymphoma type, arising de novo in a patient with preexisting Hashimoto thyroiditis or secondarily involving the thyroid in generalized lymphoma. Patients with Hashimoto thyroiditis have a relative risk of 67 of developing primary thyroid lymphoma. The transformation from Hashimoto thyroiditis to primary thyroid lymphoma occurs in about 0.5% of cases. Although most patients with thyroiditis do not proceed to lymphoma, most cases of primary thyroid lymphoma do arise in a background of thyroiditis, which accounts for approximately 60% to 90% thyroid lymphoma cases.
Thyroid lymphoma typically presents in older patients with a rapidly enlarging neck mass and obstructive symptoms such as dysphagia and dyspnea. On ultrasound, lymphomatous tissue will appear as large, solid, very hypoechoic pseudocystic masses. Posterior acoustic enhancement of the lesion is useful in suggesting the diagnosis. The diagnosis is established and distinguished from anaplastic thyroid carcinoma with fine needle aspiration biopsy and flow cytometry.
References: Rumack CM, Wilson SR, Charboneau WJ. Diagnostic ultrasound, 4th ed. Philadelphia, PA: Elsevier Health Sciences, 2011:724-726.
Stein SA, Wartofsky L. Primary thyroid lymphoma: a clinical review. J Clin Endocrinol Metab 2013;98:3131-3138.
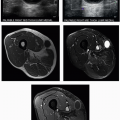
7 A 46-year-old woman with painless swelling of both parotid glands and dry mouth was referred for neck ultrasound. After reviewing her ultrasound, the most likely diagnosis is:
|

A. HIV-related lymphoepithelial cysts
B. Sjögren syndrome
C. Warthin tumor
D. Pleomorphic adenoma
View Answer
7 Answer B. The ultrasound image shows an enlarged, diffusely coarsened and heterogenous appearance of the parotid gland with innumerable small 2 to 3 mm hypoechoic lesions. These hypoechoic lesions represent areas of nonobstructive sialectasis that can be seen on sialography. These sonographic findings are characteristic of Sjögren syndrome, an autoimmune disease that causes chronic inflammation of joints, salivary glands, and lacrimal glands resulting in gland enlargement and dysfunction. Patients experience dry mucous membranes (dry mouth and dry eyes). The condition is more common in women and involves the parotid gland more frequently than it does the submandibular gland. In early stages, the parotid gland may appear normal on ultrasound. End-stage disease is characterized by gland atrophy. Ultrasound is used to monitor patients for development of lymphoma, for which they are prone.
The differential diagnosis for the ultrasound appearance includes sarcoidosis, acute sialadenitis, and granulomatous sialadenitis, which can cause diffuse heterogenous enlargement of the parotid glands, but without numerous small hypoechoic foci associated with Sjögren disease. Acute sialadenitis is painful and can be associated with clinical signs of infection, abscess formation, or calculus formation, which can be readily identified on sonography.
Lymphoepithelial cysts, Warthin tumor, and pleomorphic adenoma are benign entities that present as focal parotid lesions. Lymphoepithelial cysts present as multiple cysts in those affected with human immunodeficiency virus infection. On ultrasound, Warthin tumor and the more common pleomorphic adenoma present as circumscribed hypoechoic lesions with posterior acoustic enhancement. Both can show internal cystic change and septations. Warthin tumors are multiple or bilateral in 10% to 15% of patients.
References: Hertzberg BS, Middleton WD. Ultrasound: the requisites, 3rd ed. Philadelphia, PA: Elsevier, 2016:246.
Howlett DC. High resolution ultrasound assessment of the parotid gland. Br J Radiol 2014;76:271-277.
Onkar PM, Ratnaparkhi C, Mitra K. High-frequency ultrasound in parotid gland disease. Ultrasound Q 2013;29(4):313-321.
8a An 18-year-old woman presented to her family physician with neck swelling. Images from the thyroid ultrasound and the lateral compartment lymph nodes are provided. What are the most likely diagnosis and appropriate management?
|

A. Multinodular goiter; follow-up ultrasound in 1 year.
B. Multiple colloid cysts throughout the thyroid; no further follow-up indicated.
C. Diffuse sclerosing variant of papillary thyroid carcinoma; biopsy followed by total thyroidectomy and cervical lymph node dissection.
D. Diffuse metastatic disease to the thyroid; further imaging of the chest, abdomen, and pelvis with CT is recommended to identify a primary malignancy.
E. Chronic lymphocytic thyroiditis; thyroid function tests and supplementation with Synthroid if indicated.
View Answer
8a Answer C. The ultrasound reveals diffuse parenchymal microcalcifications throughout a mildly diffusely enlarged thyroid gland without a focal or dominant mass, typical of this more aggressive subtype of papillary thyroid cancer. Associated malignant-appearing cervical lymphadenopathy indicates the more aggressive nature of this disease.
Diffuse sclerosing variant of papillary thyroid carcinoma is an uncommon, more aggressive variant of papillary thyroid carcinoma. The thyroid cancer is manifested by numerous microcalcifications infiltrating the gland in a diffuse or regional pattern without forming a dominant mass. Pathologically, the gland reveals extensive fibrosis and numerous psammoma bodies. It is more common in females and affects younger patients, even in the pediatric population. This variant has a higher incidence of lymph node metastases but has a similar prognosis to conventional papillary thyroid carcinoma due to aggressive treatment protocols. Biopsy should be directed to an area containing microcalcifications and lymphadenopathy.
Multinodular goiter (choice A) is incorrect because there are no focal thyroid nodules. The typical appearance seen in multinodular goiter is that of multiple closely apposed solid nodules without normal intervening thyroid parenchyma.
Although differentiating tiny, bright, nonshadowing foci of microcalcifications from colloid crystals can be difficult, the lack of surrounding cystic spaces (which are often perceived with high-resolution transducers) and comet-tail artifact suggest the presence of microcalcifications. Choice B is incorrect. Psammoma bodies, which correspond to the microcalcifications seen on ultrasound, represent the most important and specific feature of papillary thyroid cancer. Cervical adenopathy will be absent in the presence of benign colloid cysts.
Metastatic disease to the thyroid is quite rare and would not show microcalcifications (Choice D). On ultrasound, metastases usually appear as solid hypoechoic nodule(s) or can diffusely replace the thyroid gland. Adenopathy can be present. Patients usually have a known diagnosis of malignancy at the time thyroid metastases are discovered because these often occur late in the disease process. Renal cell carcinoma is the most common malignancy to metastasize to the thyroid.
Chronic lymphocytic thyroiditis can cause thyromegaly and a heterogeneous, coarsened appearance of the parenchyma but is not associated with microcalcifications. Mild cervical adenopathy is characteristic, but the nodes are not frankly malignant appearing; usually, multiple mildly enlarged hypoechoic lymph nodes are located in the central compartment below the thyroid gland. Choice E is incorrect.
References: Oyedeji F, Giampoli E, Ginat D, et al. The sonographic appearance of benign and malignant thyroid diseases and their histopathology correlate. Ultrasound Q 2013;29:161-178.
Pillai S, Gopalan V, Smith RA, et al. Diffuse sclerosing variant of papillary thyroid carcinoma—an update of its clinicopathological features and molecular biology. Crit Rev Oncol Hematol 2015;94(1):64-73.
Rumack CM, Wilson SR, Charboneau WJ. Diagnostic ultrasound, 4th ed. Philadelphia, PA: Elsevier Health Sciences, 2011:716-720.
8b Which of the sonographic features listed below is most likely to be associated with a benign thyroid nodule?
A. Spiculated or lobulated nodule margin
B. Microcalcifications
C. Taller-than-wide shape
D. Extension beyond the thyroid capsule
E. Spongiform composition
View Answer
8b Answer E. Spongiform composition refers to the replacement of at least 50% of an isoechoic nodule by microcysts with intervening septa, resembling a sponge or honeycomb. Nodules with this appearance are benign with a very high specificity (99.7% to 100%). On histopathology, they represent colloid or hyperplastic nodules.
Most thyroid cancers are well differentiated, with papillary cancer being the most common thyroid malignancy, constituting 75% to 90% of all cases. Various sonographic features of thyroid cancer have been studied to help triage nodules for FNA biopsy by distinguishing suspicious from benign nodules. The sonographic features that are most specific for malignancy include extension beyond the thyroid capsule, malignant-appearing adenopathy (especially when lymph nodes contain microcalcifications or cystic degeneration), and the presence of microcalcifications (up to 95% specific). Other features of malignancy include solid and hypoechoic composition, marked hypoechogenicity (the nodule is hypoechoic relative to the strap muscle), thick and incomplete halo, spiculated or lobular margin, taller-than-wide shape, refractive edge shadowing, and interrupted peripheral calcifications. Increased central intranodular flow on color Doppler and macrocalcifications have also been associated with increased risk. Strain elastography, which measures nodule stiffness, has also been very promising in identifying malignant nodules. The more of these suspicious features are present in a given nodule, the higher the likelihood of malignancy, particularly papillary thyroid carcinoma but also medullary carcinoma.
Recently, a white paper from the American College of Radiology TI-RADS committee has proposed recommendations on risk stratification of thyroid nodules on the basis of their ultrasound appearance. The basis of the classification system entails assigning numeric points for various sonographic features of thyroid nodules; the more suspicious the feature, the more points are added to the sum. Nodules with a total score of at least 3 points are assigned a TI-RADS level 3 or higher where nodule size determines corresponding recommendations for FNA biopsy or follow up.
References: Bonavita JA, Mayo J, Babb J, et al. Pattern recognition of benign nodules at ultrasound of the thyroid: which nodules can be left alone? AJR Am J Roentgenol 2009;193(1):207-213.
Desser TS, Kamaya A. Ultrasound of thyroid nodules. Neuroimag Clin North Am 2008;18(3):463-478.
Moon WJ, Jung SL, Lee JH, et al. Benign and malignant thyroid nodules: US differentiation—multicenter retrospective study 1. Radiology 2008;247(3):762-770.
Nachiappan AC, Metwalli ZA, Hailey BS, et al. The thyroid: review of imaging features and biopsy techniques with radiologic-pathologic correlation. RadioGraphics 2014;34(2):276-293.
Oyedeji F, Giampoli E, Ginat D, et al. The sonographic appearance of benign and malignant thyroid diseases and their histopathology correlate. Ultrasound Q 2013;29:161-178.
Tessler F, Middleton W, Grant E, et al. ACR Thyroid Imaging, Reporting and Data System (TI-RADS): White Paper of the ACR TI-RADS Committee. J Am Coll Radiol 2017;14(5):587-595.
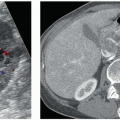
9a A middle-aged male with hyperparathyroidism underwent ultrasound and technetium-99m sestamibi scan. What is the most likely cause of this sonographic abnormality?
|

A. Renal failure
B. Parathyroid carcinoma
C. Parathyromatosis
D. Thyroid carcinoma
View Answer




9a Answer A. The ultrasound images show four oval hypoechoic nodules, two located deep to the midgland of both thyroid lobes and two others near the lower poles. The appearance, location, and delayed retention of radiotracer on technetium-99m sestamibi scan are characteristic of multigland parathyroid enlargement. Primary hyperparathyroidism is caused by autonomous production of parathyroid hormone (PTH) by a single adenoma in 80% to 90% of cases, by multiple gland enlargement in 10% to 20% cases and carcinoma in <1% of cases. On the contrary, secondary hyperparathyroidism, as present in this patient, is seen in those with chronic renal failure in which chronic hypocalcemia leads to compensatory multigland parathyroid hyperplasia. Less common causes of secondary hyperparathyroidism include osteomalacia, rickets, and malabsorption. Hyperplasia usually affects all four glands asymmetrically, whereas multiple adenomas may involve two or possibly three glands. Because distinguishing hyperplasia from adenoma is difficult pathologically and because the pattern of gland enlargement is inconsistent, when more than one parathyroid gland is enlarged, it is simply referred to as multiple gland disease.
Related posts:



Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
