Fig. 1: Position of the probe – lengthwise along the gallbladder.
Starting from the right flank, the probe is moved lengthwise along the costal arch towards the medial aspect. Viewing the margin of the liver, at the level of the medioclavicular line one observes a hypoechoic structure close to the probe – which is the gallbladder. The marker on the probe points cranially.
The following structures should be viewed:
- Gallbladder
- Vena cava (landmark!)
Landmark: vena cava
As the gallbladder is close to the probe and filled with bile, it can be visualized well in all patients. The vena cava is the landmark in this section when the gallbladder has been removed. When the gallbladder is covered by the shadow of a rib, it may help to let the patient inhale deeply or position the probe in the intercostal space.
The gallbladder varies markedly in terms of its position, size and shape, and also differs according to the time point of the patient’s last meal. A “fasting” gallbladder is well filled, hypoechoic, and has a tender wall (Fig. 2 a). Postprandially it is contracted, slightly smaller, more narrow, and has a three-layered wall (Fig. 2 b).
The position, size and shape may vary significantly.
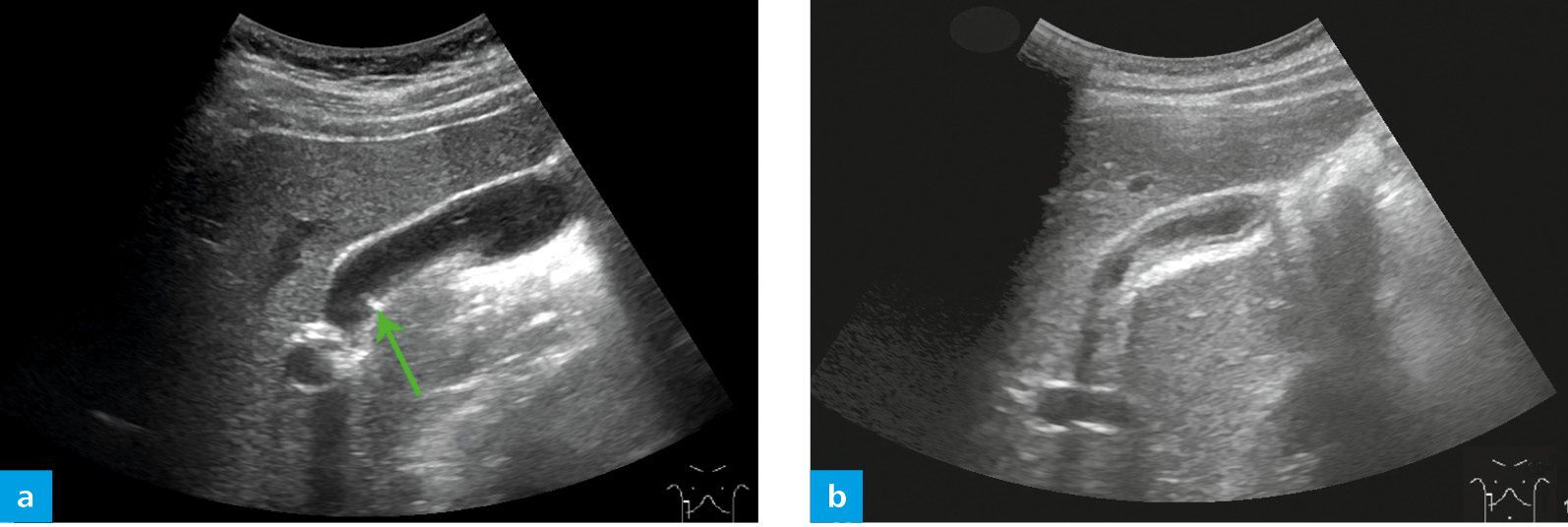
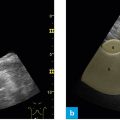
Fig. 2: Filled gallbladder with a tender wall (a), contracted gallbladder with a layered wall postprandially (b).
Hyperechoic, hypoechoic and hyperechoic” layers in a contracted postprandial gallbladder should not be confused with a pathology. One may even observe a small septation or kinking (Fig. 2 a, green arrow) of the gallbladder.
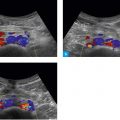
Clinically one should pay special attention to gallstones which, in contrast to polyps, are accompanied by an acoustic shadow. An inflamed gallbladder is marked by significant parietal thickening and intensified vascularization.