7 7.1 Filling defect in the gallbladder 7.3 Thickened gallbladder wall > 3 mm – excluding the physiological, contracted (empty) gallbladder. 7.4 Gas in the biliary tract 2. Emphysematous cholecystitis – due to gas-forming organisms and associated with diabetes in 20% of cases. There is intramural and intraluminal gas but, because there is usually cystic duct obstruction, gas is present in the bile ducts in only 20%. The erect film may show an air–bile interface. 7.5 Gas in the portal veins 1. Bowel infarction – the majority of patients die soon after gas is seen in the portal veins. 5. Air embolus during double-contrast barium enema – this has been observed during the examination of severely ulcerated colons and is not associated with a fatal outcome. 6. Acute gastric dilatation – in bed-ridden young people. May recover following decompression with a nasogastric tube. 7.8 Hepatic calcification 1. Hydatid – liver is the commonest site of hydatid disease. Most cysts are in the right lobe and are clinically silent but may cause pain, a palpable mass or a thrill. 20–30% calcify and, although calcification does not necessarily indicate death of the parasite, extensive calcification favours an inactive cyst. Calcification of daughter cysts produces several rings of calcification. 2. Abscess – especially amoebic abscess when the right lobe is most frequently affected. 3. Calcified (porcelain) gallbladder – strong association with gallbladder carcinoma. 1. Metastases – calcification is uncommon but colorectal and gastric carcinomas calcify most frequently. It may be amorphous, flaky, stippled or granular and solitary or multiple. Calcification may follow radiotherapy or chemotherapy. 2. Fibrolamellar hepatocellular carcinoma – usually small, centrally located and only visible on CT. 3. Adenoma – rare. Calcifications are punctate, stippled or granular. Often placed eccentrically within a complex heterogeneous mass.
Gallbladder, liver, spleen and pancreas
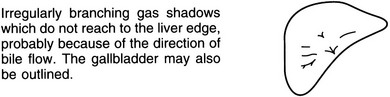
Within the bile ducts
Spontaneous biliary fistula
Within the gallbladder
Curvilinear
Localized in mass
Radiology Key
Fastest Radiology Insight Engine