Gastrointestinal & Hepatobiliary Scintigraphy
James Connelly
Jan Fjeld
Mona-Elisabeth Revheim
LEARNING OBJECTIVES
1. Describe methods to investigate gastrointestinal (GI) function in different parts of the GI tract.
2. List commonly used gastrointestinal and hepatobiliary track tracers.
3. Describe methods to investigate specific types of GI pathology including salivary gland diseases, gastroesophageal reflux, Meckel’s diverticulum, GI bleed, protein loss enteropathy, biliary acid recirculation.
4. List different ways hepatobiliary scintigraphy can be used to image different clinical indications.
5. Describe tracers and methods to identify and image different aspects of liver and splenic tissue.
GASTROINTESTINAL FUNCTIONAL STUDIES
Gastrointestinal symptoms can be diffuse, nonspecific, and difficult to pinpoint due to the length and motile mature of the gastrointestinal tract and correlation between the different regions. Nuclear medicine provides a relatively physiological approach to image all or part of the gastrointestinal tract during consumption of a meal and its progress through the esophagus, stomach, small-bowel, colon, and excretion. Usually, the investigation is truncated to the part of the GI tract most affected, with gastric emptying being the most frequently performed investigation. However, it is worth remembering that regional motility is dependent on both input and output, so some representation of this should be included in the imaging study. There is close relationship with radiological and endoscopic techniques. Whereas nuclear medicine does not provide the anatomical detail of the other methods, it provides a complementary overview and slow dynamic imaging methods that are not really practical with X-ray, compute tomography (CT) or even magnetic resonance (MR).
GASTRIC EMPTYING SCINTIGRAPHY
Abnormal gastric emptying may be a consequence of various diseases, leading to either too slow or too fast emptying rate. Symptoms and signs indicating gastric emptying problems are difficult to interpret, and the problem is frequently psychologic. Therefore, objective method for assessment of gastric emptying is a necessity. With a radiolabeled meal and dynamic scintigraphy, it is easy to assess gastric emptying.
The emptying rate is highly dependent on the meal. Therefore, standardized meals must be used, and reference intervals for these meals must be established (1). Moreover, there is a relatively broad biologic variation in gastric emptying rate, which leads to wide reference intervals also when standardized meals are used (2). For a person with an emptying rate close to the center of the normal reference interval for a specific meal, a relatively large deviation from the normal rate is necessary to avoid a false-negative result.
Nuclear medicine test methods with solid food are considered the gold standard for measuring gastrointestinal emptying, but emptying studies with liquids are also of interest, especially in small children and patients fed through various types of tubes. The examination can be modified into a double isotope method with a mixture of differentially labeled solid food and liquid, for example, 111In-DTPA in water that is drunk with the solid test meal labeled with 99mTc-DTPA. The usefulness of this, however, seems limited.
Delayed emptying is seen with mechanical hindrances in the pylorus (cancer or ulcer with stenosis), diabetes mellitus with autonomic neuropathy, hypothyroidism, after a vagotomy, in collagen diseases, amyloidosis, uremia, anorexia, and depression, as well as idiopathic. Aberrant rapid emptying may be seen after gastric surgery, in patients with Zollinger-Ellison syndrome, carcinoid syndrome, duodenal ulcers, hyperthyroidism, and diabetes in the early phase.
SCINTIGRAPHIC PRINCIPLE
Radioactivity, most often a 99mTc-labeled radiopharmaceutical, is added to a standardized meal (3). The radiopharmaceutical added must be of a kind that is not absorbed from the gastrointestinal tract, and it must follow the test meal within the gastrointestinal tract. Examples are 99mTc-labeled sulfur colloid or DTPA. After intake of the test meal, the gastric emptying rate is measured by dynamic scintigraphy from time of intake and for the next 60 or 90 min, and sometimes for a longer period if the emptying is slow.
Indications
Unexplained dyspepsia
To detect or exclude gastroparesis, most often in patients with type 1 diabetes and autonomic neuropathy
Verify dumping syndrome
Detection of gastroesophageal reflux
Following up previously detected motility disorders Contraindication, special precautions, side effects
There are no special contraindications. Side effects are not described. Breastfeeding can continue without interruption.
GENERAL STUDY PROTOCOL
The patients are instructed to fast without food and drinks for at least 4 h, preferably 8-h fast overnight. To be scheduled for investigation, the next morning is most convenient in combination with an overnight fast.
Diabetics should postpone their morning insulin until after the test meal. Early morning doses of drugs that affect the stomach’s emptying should, if possible, be brought along and taken immediately after the investigation. Opiates, calcium blockers, anticholinergics, antidepressants, levodopa, histamine H2-antagonists, proton pump inhibitors, and antacids with aluminum tend to slow down the emptying rate. Erythromycin, metoclopramide, and cisapride increase the emptying rate.
Body mass index (BMI), age, and a history of smoking are of marginal significance to gastric emptying. However, emptying will depend on the volume of the meal and its composition, if the meal is solid or a liquid, and whether the person is standing, sitting or lying down. Hence, one must therefore strive for identical testing conditions, including standardization of the composition of test meals. A variety of standard meals are used. Eggs and bread are frequently used. With egg meals, only the egg white may be used. The yolk has a high content of fat and calories, and both these factors may reduce the emptying rate. Egg white from two eggs scrambled in the microwave oven and put between two halves of a slice of white bread is used by these authors for adult patients. The 99mTc-sulfur colloid is added to the egg white before the heating procedure.
Individual adaptation of meal volumes or composition in relation to allergies or other illnesses, or administration routes, should be evaluated by a physician for best possible administration. Children, dependent on age, drink 150 mL of cow’s milk or other liquid nutrition, or solid food as for adults, in reduced amount. For tubefed patients, the tube position in the stomach must be verified. The intake phase should be finished within maximum 10 min.
Camera recording should start immediately after the meal has been finished. Dynamic registration is performed over the abdominal area:
Simultaneously, front and rear imaging, with a two-headed camera and calculating the decay-corrected geometric average.
In addition to the stomach, the lower part of the esophagus, and the duodenum and the upper part of the small intestine, must be in the field of view.
Time: approx. 90 min (5400 s), typically 90 s per image.
For very restless children, one can take static images at regular intervals (approximately every 10 min). If the only camera available has one detector, the left anterior oblique (LAO) projection is preferable to anterior (ANT) projection. It may be appropriate to follow up with more images throughout the day. Static images should be taken in 256 × 256 format every 10 min or so.
It is important with some anatomical landmarks on these scintigrams with very little anatomy except for the gastrointestinal tract, for example by marking right shoulder.
INTERPRETATION AND REPORTING
After ingestion, solid food will remain for some time in the stomach. In this lag period or plateau phase, peristalsis prepares the food for emptying to the duodenum. Then an exponential fall in radioactive gastric content following a solid meal is observed. Men, and women after menopause, have a somewhat faster gastric emptying than premenopausal women. But this gender difference is small, and separate reference ranges are not necessary. The difference in emptying between the different patients groups is frequently due to a different length of the initial plateau phase.
Compared with solid food, the liquid test meals are poorer at discriminating between normal and pathological emptying. Different liquids may also differ in their emptying rate. The emptying immediately after intake, with no plateau phase, and there is no significant difference between genders. In adults, the normal half-life is 10 to 60 min. In children, there seems to be a particularly large difference in emptying patterns depending on the volume of milk ingested and methodology in general. Breast milk and water are emptied exponentially, as with liquid test meals in adults, while test meals of cow’s milk or infant formula often have long plateaus. Rectilinear fall with an immediate start can also be seen. Generally applicable reference values for children are lacking.
If gastrointestinal emptying examinations are carried out consistently, the emptying parameters will be reasonably well reproduced with a variation coefficient of about 15%. Patient movement bringing the stomach completely or partly outside the region of interest (ROI) is a source of error, which can be corrected and can easily be observed if the scintigrams are displayed dynamically in connection with processing. The overlap between gastric ROI and small intestine activity is another source of error.
As many practices are performing 4-h gastric emptying studies, it is useful to remember the upper limit of normal at two standard deviations above the mean forgastric retention as: (1 h: 90%; 2 h: 60%; 3 h: 30%; 4 h: 10%)
GASTROESOPHAGEAL REFLUX AND PULMONARY ASPIRATION
The two main problems with gastrointestinal reflux are esophagitis and pulmonary aspiration. Like in gastrointestinal emptying, dynamic scintigraphy is also well suited for monitoring if an ingested meal takes a retrograde course from the stomach into the esophagus, and further into the lungs.
Pulmonary aspiration might happen in situations with reduced consciousness after trauma or anesthesia or due to a reduced gag reflex. However, the cases suitable for scintigraphic investigation are those with a confirmed gastroesophageal reflux, and suspected to have a lung problem caused by aspiration of acidic ventricular content. Most patients with this problem are children (4).
Various investigations outside the nuclear medicine field are applied on patients suspected of having a gastric reflux problem. An X-ray examination using contrast of the upper gastrointestinal tract can detect underlying abnormalities in the esophagus, stomach, and duodenum, as well as demonstrating esophageal motility. A Meckel’s scintigraphy can detect Barrett’s esophagus with ectopic epithelium. Endoscopy and an esophagus biopsy can be used to detect esophagitis. The gold standard for reflux detection is 24 h of pH measurement in the esophagus. A fall in acidity below pH 4 for more than 4% in a 24-h period is considered pathological.
Scintigraphic examinations of gastroesophageal reflux are not invasive and produce a very low radiation dose. Sensitivity to detection of reflux is highest with patients in supine position, and equivalent to the sensitivity of pH measurement in the esophagus. The method’s main limitation is that the examination period is necessarily short. It is not possible to monitor the patient throughout the whole day and night. Nevertheless, scintigraphy is probably the most effective method available for detecting pulmonary aspiration (5).
Scintigraphic principle
A 99mTc-labeled radiopharmaceutical that is not absorbed from the GI-tract is added to a test meal. After intake of the test meal, gastric emptying is measured by dynamic scintigraphy, with lungs and upper part of the abdomen within the camera field of view. Hence, gastric emptying, reflux to the esophagus and aspiration will be revealed.
Indications
Confirmation of gastroesophageal reflux
Clarify if lungs problems are due to aspiration of gastric content
Contraindications
There are no special contraindications. Side effects are not described. Breast feeding can continue without interruption.
General study protocol
The investigation should start in the morning, after the patient has eaten breakfast. Hospitalized patients are studied with juice or milk (at least 150 mL). Children are given 10 mL of juice, milk, or a nutrition liquid with 10 MBq 99mTc-DTPA, followed by as much as possible of the nonradioactive juice/milk/nutrition. Infants should have a feeding bottle with milk or other kind of nutrition that they are usually fed with. Adults are given 75 mL of fluid with 10 MBq 99mTc-sulfur colloid and then 75 mL fluid without radioactivity. The patient should sit on a chair with the camera posteriorly over the thorax. Dynamic registration is performed for a total time of typically 60 s, 1 s per image. Then, after drinking, the patient lays down on their back for a dynamic registration posteriorly over the thorax, typically for a total of 2700 s (45 min), 30 s per image.
It is important to add an anatomic landmark to the images to know where the radioactive test meal is located within the gastrointestinal tract. The patient can eat and drink normally after the examination. If the indication for the examination is reflux into the lungs, an extra static image in front and back view of the thorax is appropriate later the same day, and the next morning as well. By following the ROI of the stomach and esophagus during a recording period of approximately 45 min, a time activity curve will give indication whether reflux is present or not. The static images will also add valuable information.
Interpretation and reporting
Almost all children have gastroesophageal reflux the first weeks of life. Some show symptoms, but the symptoms usually disappear when a child reaches 12 months of age. Persistent reflux can cause eating discomfort and “failure to thrive,” and can also cause respiratory symptoms, including aspiration pneumonia and asthma. The normal transit period through the esophagus is 6 to 15 s. Any reflux is graded according to duration and proximal extent. Short-term gastroesophageal reflux into the lower part of the esophagus is not to be regarded as abnormal, but detectable pulmonary aspiration is clearly pathological.
No sign of focal activity in the lungs on late scintigrams does not exclude aspiration because the patient may have coughed up aspirate or insufficient amount of activity was left in the stomach during reflux and aspiration. Further imaging has no value when the stomach is completely empty. Scintigraphy cannot replace an X-ray contrast examination when the representation of anatomical details is of interest or necessary.
SMALL BOWEL AND COLON TRANSIT STUDIES
Small and large bowel investigations are performed as a modified continuation of gastric emptying studies(6). Intestinal transit studies have been around for a while but frequently done in a multitude of different ways. To promote more standardized practice, a joint guideline was issued by the society of nuclear medicine and molecular imaging (SNMMI) and European Association of Nuclear Medicine (EANM) in 2013 (7).
Indications
Suspected gastroparesis
Dyspepsia
Irritable bowel syndrome
Chronic constipation, chronic diarrhea
Chronic idiopathic intestinal pseudo-obstruction
Scleroderma
Celiac disease
Malabsorption syndromes
Procedure
Preparation for intestinal transit is the same as for gastric emptying (which is the starting point for the investigation):
Note food allergies/intolerances
Fast overnight or a minimum of 8 h
Review medication in advance and discontinue medications that influence motility at least 48 to 72 h in advance (medications that slow transit such as opioids and anticholinergics and prokinetic medications, e.g., erythromycin, laxatives) unless this is an assessment intended to be on ongoing or subsequent treatment.
Diabetic patients should aim to be euglycemic.
Normal diet 2 days before and during the 4 to 6 days of a colon study.
Protocols
The following procedures are recommended:
Two tracers, 99mTc and 111In; 67Ga is an alternative to indium but infrequently used.
Options of either (A) whole-gut transit (including gastric emptying, small bowel and colon transit), (B) small bowel transit (without the colonic section), or (C) colon transit study. The main difference between the methods is option B stops after 24 h, options A and C involve imaging up to 72 h or longer.
The two tracers allow two protocols for each option, either as a single or as a dual isotope method. In all protocols, the small bowel and colonic study is done with a labeled water phase (111In-DTPA, unless single-phase small-bowel transit only, for which 99mTc-DTPA can be used) and with a solid phase that may be labeled with 99mTc-DTPA. In practice, this means 300 mL of labeled water and a standard meal (and for solid gastric emptying: egg white omelet, 2 slices white bread, 30 g strawberry jam,
120 mL water). There is one exception. For colon transit, an enteric-coated capsule containing 111In-activated charcoal particles that dissolves in the small bowel and delivers a bolus of activity in the terminal ileum have been established, however, the capsule is not generally available.
120 mL water). There is one exception. For colon transit, an enteric-coated capsule containing 111In-activated charcoal particles that dissolves in the small bowel and delivers a bolus of activity in the terminal ileum have been established, however, the capsule is not generally available.
 FIG. 12.1 • Gastric emptying and small bowel transit in a patient following a 99mTc-labeled solid meal. (A) Analysis showing curves derived for regions of interest over the stomach and small bowel for the first 2 h using a dynamic imaging protocol. (B) Hourly images mapping the progression of tracer through the small bowel and into the terminal ileum at 5 h and cecum at 6 h. |
The general imaging procedure is based on the whole-gut transit study.
Large field of view, medium energy collimator for 111In ±99mTc, 128 × 128 matrix.
A cobalt positioning marker on the iliac crest for anatomical reference.
Anterior and posterior images for 1 min at hourly intervals for 6 h for both 111In-DTPA or 99mTc-DTPA liquid phase methods.
If there is a 99mTc-labeled solid phase, then the gastric emptying imaging protocol is used initially up to 4 h.
Further images for 4 min at 24, 48, and 72 (and more if necessary) h for 111In. If 99mTc-DTPA is used for small bowel transit, then only additional imaging is performed up to 24 h.
Correction is made for isotope decay.
Image analysis
Small bowel transit starts as a gastric emptying investigation then maps the progress of tracer through the small bowel until it reaches the terminal ileum and transfers into the cecum, typically within 6 h of the meal.
An example of a gastric emptying study together with a small bowel uptake curve over 2 h is shown in Figure 12.1A followed by hourly imaging up to 6 h in Figure 12.1B. The images show normal emptying and progression through the small bowel. A quantitative measure of the small bowel is the small bowel transit index at 6 h that measures the total counts in the terminal ileum and colon divided by the average total abdominal counts on the 2 to 5 h images. Geometric mean decay counts are used. Table 12.1 shows reference values for studies based on the guideline protocol.
Potential errors in assessment can arise in identifying the terminal ileum and cecum. The terminal ileum has a reservoir role so transfer to the colon occurs at a different rate, and an image at 24 h is a useful check to see if there is normal transfer to the cecum and that a more proximal hold up has not been misinterpreted as the terminal ileum. Slow transit to the cecum may also be secondary to delayed colonic transit
Table 12.1 REFERENCE VALUES FOR SMALL BOWEL AND COLON TRANSIT TIMES (FROM [7]) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|
|
Colon transit assessment ideally follows a bolus of activity from the cecum to excretion and is the motivation for a capsule method where the tracer is released in the terminal ileum. The capsule method is not generally available so the protocol begins with combined standard meal and 111In-DTPA water and follows hourly and then daily imaging as previously described. Analysis is based on measuring geometric mean counts in segments of the colon, corrected for decay and normalized to the initial total abdominal counts. Typically, five or seven segments are defined. Counts in each segment can be given as percentage of the total or as a geometric center value, calculated by multiplying the fraction of the total counts in a segment by a weighting factor according to how distal the segment is in the colon and summing over all segments. Figure 12.2 shows analysis of a normal colonic transit case.
There are three main abnormal patterns of slow colonic transit. Generalized slow transit is typically characterized by delayed progression with widespread retention of tracer involving multiple segments. A case is shown in Figure 12.3A. Colonic inertia is rather characterized by delayed accumulation of tracer before the splenic flexure. Functional outlet obstruction is where there is accumulation of tracer in the rectosigmoid region but without proportionate excretion. Figure 12.3B shows a case of rectosigmoidal delay, although relatively normal total colonic transit. By using standardized protocols, reference values can provide useful guidance. These protocols and reference values should either be defined carefully locally or follow established guidelines.
 FIG. 12.2 • Colonic transit study using 111In-DTPA demonstrating segmental analysis (ascending, transverse, descending, rectosigmoid, and excretion segments) showing percentages of total activity in each segment. Normal transit. |
There are potential a plethora of factors that can affect bowel transit including medication, past surgery, lesions, and age. Transit studies form part of a panel of procedures and investigations to identify the underlying cause and provide only one piece of the usually much larger diagnostic jigsaw associated with bowel pathology.
SALIVARY GLAND FUNCTION
The salivary glands consist of three pairs of exocrine glands. The largest are the parotid glands located immediately posterior to the mandibular ramus with a duct that extends forward and opens into the mouth in the mid buccal region. The second largest are the submandibular glands that are placed medially to the posterior lower edge of the mandibular. The ducts from these glands extend anteriorly to exit through sublingual caruncles either side of the frenulum. Finally, the sublingual glands are located anteriorly submucosally in the floor of the mouth and also drain either side of the frenulum.
Salivary gland scintigraphy was established as a method in the 1970s. There are a number of different protocols described
in the literature. Most are aimed at semi-quantitation of function to evaluate the degree of xerostomia (dryness of the mouth) (8).
in the literature. Most are aimed at semi-quantitation of function to evaluate the degree of xerostomia (dryness of the mouth) (8).
 FIG. 12.3 • Colonic transit study using 111In-DTPA demonstrating (A) generalized slow transit, (B) recto sigmoidal delay. |
A dynamic scan following intravenous injection of 99mTc pertechnetate allows uptake of tracer into the salivary glands to be followed. Uptake is assumed to be proportional to glandular function. To assess excretion, lemon juice is given toward the end of the registration to stimulate salivary glands to empty. This also allows the drainage conditions to be evaluated.
Indications
Sjøgren’s syndrome to estimate grade of xerostomia grade
Infectious (viral/bacterial) sialadenitis
Saliva stone or suspected obstructed salivary gland for some other reason
Grading of radiation damage (radioiodine induced or due to external radiation therapy)
Unexplained dry mouth
Contraindications
Allergic reaction has been described, but is extremely rare
Check that the patient has not had recent X-ray contrast, iodine supplements, perchlorate thyroid protection (last 24 h) or is on medication that have dry mouth as a significant side effect.
It is not usually necessary to do this investigation during pregnancy or while breastfeeding. The European Nuclear Medicine Guide (9) suggests breastfeeding must be interrupted for 12 h and pumped milk during that time should be discarded.
PROTOCOL
Gamma Camera with Low Energy, High-Resolution Collimator (LEHR)
The patient should fast for an hour before the test.
The patient is placed under the camera with the head in a headrest and as far back as possible. 185-370 MBq 99mTc pertechnetate is given intravenously.
Dynamic registration in AP position, zoom × 2, 128 × 128 format, 20 s per image for 50 min. The patient is asked not to swallow unnecessarily during the examination.
After 40 min, the patient is given 2 mL of concentrated lemon juice using a plastic pipette to ensure minimal head movement. The patient holds the lemon juice in the mouth 15 to 20 s before swallowing. Imaging continues for a further 10 min.
Effective dose 4.7 mSv/370 MBq. The colon and thyroid gland receive the highest equivalent dose.

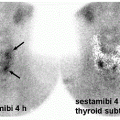
FIG. 12.4 • Salivary gland scintigraphy. Normal uptake is shown in A and B. (A) Summed uptake of all images defining regions of interest (ROI) over the parotid glands (region 1 and 2 red/green), over the salivary glands (ROI 3 & 4 blue/purple) and background (ROI 5, white). (B) Time activity curves for each ROI. Lemon juice is given after 2400 s (vertical red dotted line). C & D show a patient treated for thyroid carcinoma with postradiation xerostomia and are processed as in A & B. There is considerable reduced tracer uptake by the glands, virtually negligible in the parotid glands, and no significant excretion stimulated by lemon juice.
The images are processed by defining five oval regions of interest placed over the oral cavity and the four major salivary glands, respectively, as well as two smaller background regions temporally and sub mentally, respectively, near the parotid and submandibular glands, as shown in the Figure 12.4. Time activity curves are produced for each gland.
Parameters such as the ejection fraction post lemon juice stimulation, visual appearance scores, uptake curve parameters, and excretion time intervals can be measured and used as objective measures of xerostomia and to follow progression over time.
Applications
Salivary gland scintigraphy is almost always used in conjunction with radiological techniques and frequently after biopsy, so the diagnosis is known. It primarily provides a means to assess function.
Normal uptake and secretion are demonstrated in Figures 12.4A and 12.4B. Figures 12.4C and 12.4D show a patient with xerostomia after treatment for thyroid carcinoma and subsequent metastatic recurrence with two courses of radioactive iodine. There is virtually no tracer uptake in the parotid glands, which were atrophied on CT and ultrasound. There is also significantly
reduced uptake in the submandibular glands with no response to lemon juice stimulation. Studies suggest that the parotid gland is more susceptible to radiation damage, that subjective dry mouth symptoms are more strongly associated with submandibular gland dysfunction and that there is a dose-response relationship between radiation dose and salivary dysfunction parameters.
reduced uptake in the submandibular glands with no response to lemon juice stimulation. Studies suggest that the parotid gland is more susceptible to radiation damage, that subjective dry mouth symptoms are more strongly associated with submandibular gland dysfunction and that there is a dose-response relationship between radiation dose and salivary dysfunction parameters.
Oral cavity activity parameters are also useful to discriminate between normal and patients with different stages of Sjøgren’s syndrome (8).
The largest source of error arises from inconsistency in the instillation of lemon juice. Less significant is competitive inhibition of the tracer by other sources of iodide, for example, X-ray contrast, food supplements, or similar anions such as perchlorate used in other nuclear medicine investigations to block or protect the thyroid.
MECKEL’S SCINTIGRAPHY
Meckel’s diverticulum is a congenital diverticulum in the ileum, with an incidence of 2%. Most people go through life without any problems related to it, not even knowing that they were born with this anatomic variation, and only 25% to 40% of them will experience symptoms from this diverticulum localized 50 to 100 cm from the ileocecal valve. As 25% of the diverticula contain heterotopic gastric mucosa, this congenital defect may be the origin of a gastrointestinal bleed. This is most common in childhood, and most frequently before the age of 5 years. Less frequently, a Meckel’s diverticulum may also lead to complications like diverticulitis, obstruction, or perforation. These complications are more common in adult patients. It is very seldom that patients presenting with Meckel-related complications are over the age of 40.
Scintigraphic principle
In addition to the thyroid and salivary glands, 99mTc-pertechnetate is concentrated in gastric mucosa cells, and the goal of scintigraphy is to look for ectopic gastric mucosa, i.e., not the bleeding per se. The typical patient is an otherwise healthy child suspected of intestinal bleeding before the age of 5 years, most often less than 2 years. Within this relatively rare group of children with a gastrointestinal bleed a Meckel’s diverticulum with ectopic gastric mucosa is a frequent explanation for the situation.
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


