Air bronchogram.
Air crescent sign.
Silhouette sign.
Cervicothoracic sign: An intrathoracic mass whose cranial border is seen to project on posteroanterior (PA) radiographs superior to the clavicles must be located dorsally since the posterior portions of the lung apices extend farther cranially than their anterior counterparts.
Extrapleural sign: A mass arising from the chest wall, pleura or mediastinum which on a radiograph exhibits a blurred, ill-defined border with tapered margins and an obtuse angle, whereas an intrapulmonary lesion has a more defined border and acute angle. For more information, please consult Section 11.5 and ▶Fig. 11.9.
Gloved finger sign: Dilated, mucoid-impacted bronchi that on radiographs manifest as gloved fingers. This sign is typically observed in allergic bronchopulmonary aspergillosis and mucoviscidosis. But it can also present concomitantly with myriad other diseases secondary to longstanding central bronchial obstruction.
Golden S sign: This refers to the lateral bulging of a central tumor secondary to lobe atelectasis; see ▶Fig. 9.15. The resultant reverse S shape was initially used by R. Golden only to describe the external contour of the atelectatic area of the right upper lobe,2 but this can also be applied to other lobes.
Table 3.1 Causes of unilateral changes in thoracic radiolucency on radiograph
Maximum decrease in unilateral radiolucency: “white-out hemithorax”
Large pleural effusion (see ▶Fig. 3.1)
Volume increase
Total atelectasis (see ▶Fig. 3.2)
Volume reduction
Pneumonectomy
Volume reduction, possibly surgical clips in mediastinum and hilum
Unilateral decrease in radiolucency
Pleural effusion (in particular, posterior on supine images)
Ultrasound
Pneumonia
Inflammatory biomarkers
Lung carcinoma
Volume increase
Pleural carcinosis
Volume increase
Pleural mesothelioma
Volume reduction
Thoracoplasty
Calcifications, thoracic deformity
Unilateral increase in radiolucency
Congenital lobar emphysema
Massive hyperventilation of the deceased lung lobe
Swyer-James syndrome
Vascular rarefaction
Foreign body
Air trapping due to valve mechanism
Central lung carcinoma
Rarely, air trapping due to valve mechanism, more commonly atelectasis
Deep sulcus sign: This refers to the abnormal increase in radiolucency seen on supine radiographs, originating from a costophrenic angle (sulcus) and extending into the lateral portions of the adjacent upper abdominal quadrant. This sign is indicative of anterior pneumothorax.

 Fig. 3.1 Large right-sided pleural effusion. Radiograph. Mediastinal displacement to the left. Total compression atelectasis of the right lung. |
Table 3.2 Causes of atelectasis | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Right upper lobe atelectasis (▶Fig. 3.3): The right upper lobe collapses in a cranial and mediastinal direction. This, in turn, causes cranial displacement of the minor (horizontal) fissure, in particular, of the lateral portion. It also results in a high-riding diaphragm on the right. If atelectasis is caused by a central tumor, the tumor can at times be identified as bulging of the external contour of the atelectatic area, known as the Golden S sign.
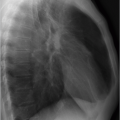
Middle lobe atelectasis (▶Fig. 3.4): The middle lobe collapses in an inferoposterior direction. On PA radiographs, this is seen as an upward directed, smoothly marginated opacity, whereas on lateral views it manifests as anterobasal triangular opacity.

Fig. 3.2 Total atelectasis of the left lung secondary to central lung carcinoma. Radiograph. Lung metastasis in right upper lobe (arrow).

Fig. 3.3 Right upper lobe atelectasis. Radiograph. Atelectasis can be clearly identified on the PA radiograph (arrows).
 Fig. 3.4 Middle lobe atelectasis. Radiographs. Atelectasis can be clearly identified on the lateral view (b, arrows). (a) PA image. (b) Lateral view. |
 Fig. 3.5 Right lower lobe atelectasis. Radiograph. Atelectasis can be clearly seen on the PA radiograph (arrows).
Related posts:Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|