, Joungho Han2, Man Pyo Chung3 and Yeon Joo Jeong4
(1)
Department of Radiology Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea, Republic of (South Korea)
(2)
Department of Pathology Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea, Republic of (South Korea)
(3)
Department of Medicine Division of Pulmonary and Critical Care Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea, Republic of (South Korea)
(4)
Department of Radiology, Pusan National University Hospital, Busan, Korea, Republic of (South Korea)
Abstract
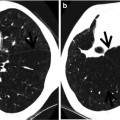
Gloved finger sign is originally described on chest radiography and represents mucoid impaction of the branching bronchi [1]. The sign is formed by branching tubular, toothpaste, or fingerlike densities [2]. On CT, the dilated bronchi, filled and impacted with mucus (usually fluid attenuation but variable depending on the constituents of content in the dilated bronchi), generate a gloved finger appearance [3] (Fig. 10.1).
Definition
Gloved finger sign is originally described on chest radiography and represents mucoid impaction of the branching bronchi [1]. The sign is formed by branching tubular, toothpaste, or fingerlike densities [2]. On CT, the dilated bronchi, filled and impacted with mucus (usually fluid attenuation but variable depending on the constituents of content in the dilated bronchi), generate a gloved finger appearance [3] (Fig. 10.1).
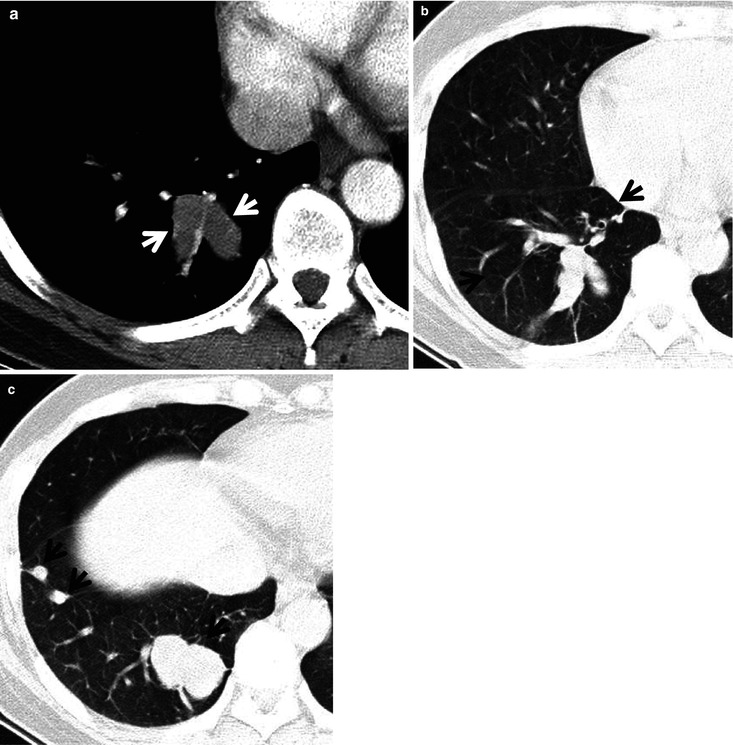
Fig. 10.1
Bronchial atresia showing gloved finger appearance in a 43-year-old woman. (a) Mediastinal window image of enhanced CT scan (5.0-mm section thickness) obtained at level of the suprahepatic inferior vena cava shows V-shaped low-attenuation lesion (arrows) in the right lower lobe. (b) Lung window image of CT scan obtained at similar level to (a) demonstrates same branching lesion. Please note low-attenuation area (arrows) surrounding branching lesion. (c) CT scan obtained at level of liver dome displays branching nodular lesions (arrows) in the right lower lobe
Diseases Causing the Sign
Any airway obstructive lesions may result in gloved finger sign. Benign and malignant neoplasms (Fig. 10.2) causing airway obstruction can cause distal bronchiectasis and mucoid impaction. Developmental airway disease, bronchial atresia (Fig. 10.1), usually appears as gloved finger sign. Broncholithiasis, bronchial tuberculosis and stricture (Fig. 10.3), intralobar pulmonary sequestration, and foreign-body aspiration may also cause mucoid impaction and gloved finger sign. Allergic bronchopulmonary aspergillosis (ABPA) (Figs. 10.4 and 10.5) and cystic fibrosis with or without ABPA are the two most common nonobstructive diseases causing gloved finger sign on radiologic examinations [2] (Table 10.1).
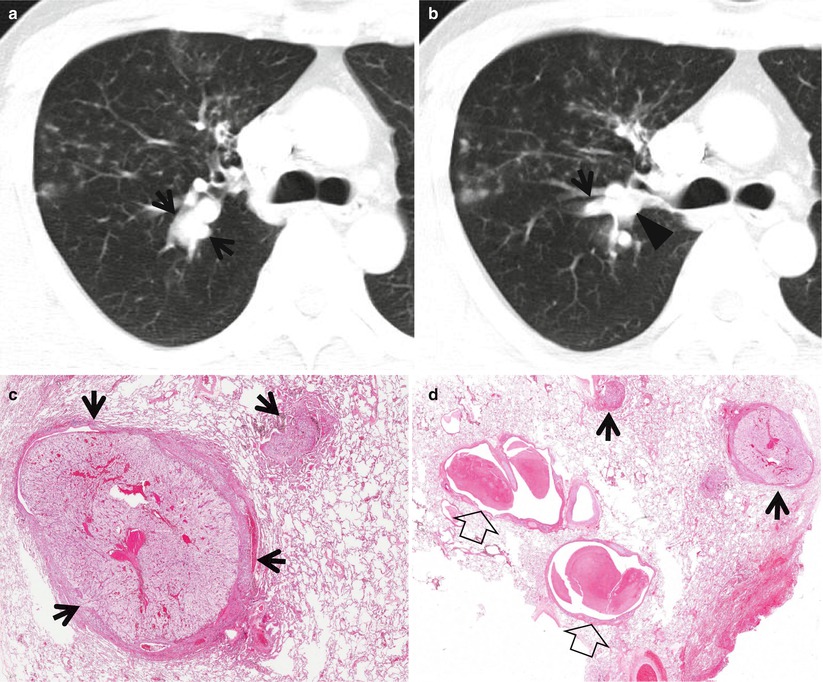
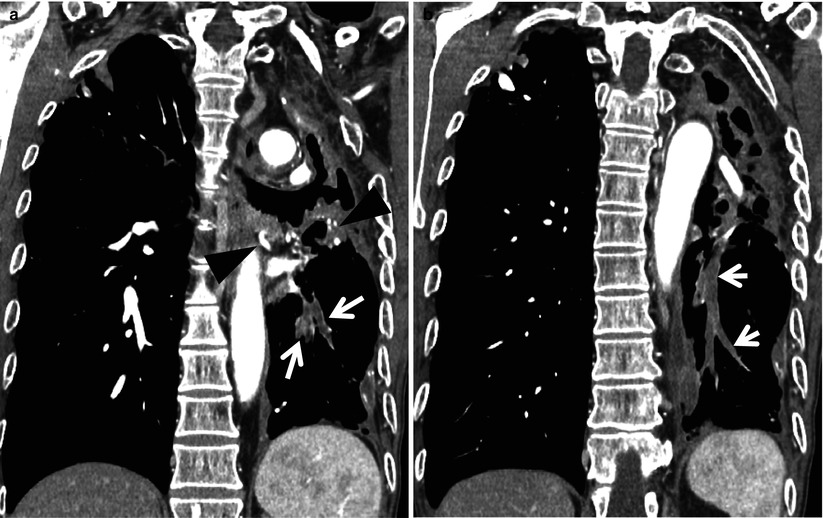
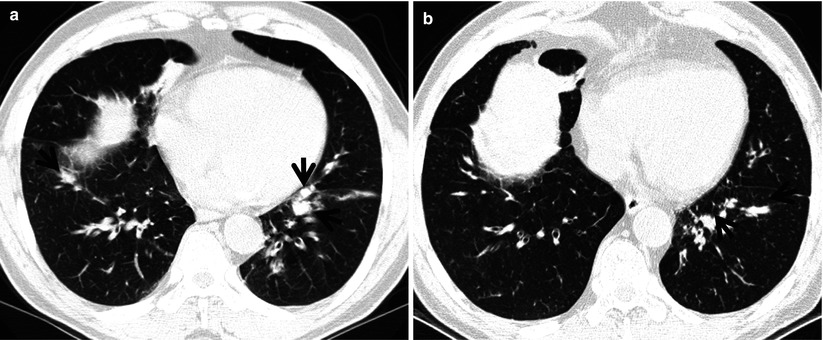
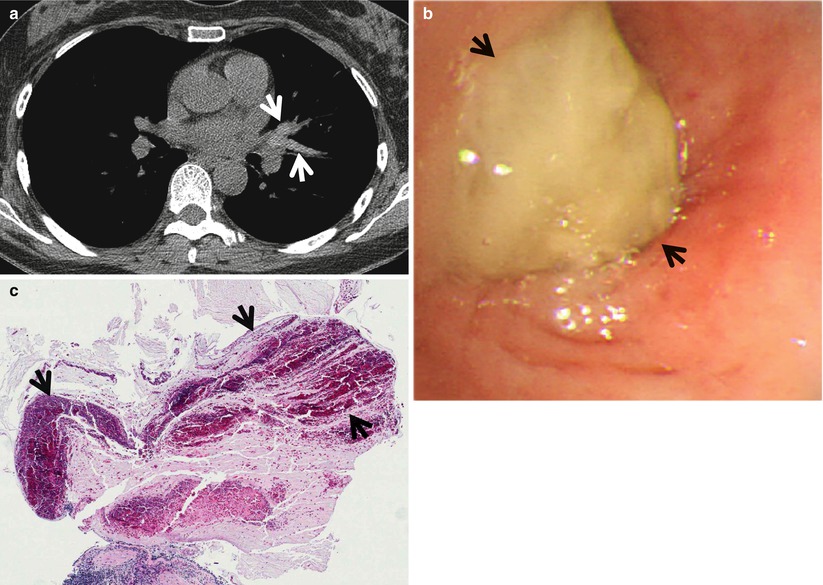
Fig. 10.2
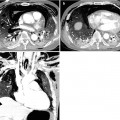
Gloved finger sign associated with mucus retention in airways distal to endobronchial metastasis in a 54-year-old man with renal cell carcinoma. (a, b) Lung window images of CT scans (5.0-mm section thickness) obtained at levels of the azygos arch (a) and main bronchi (b), respectively, show branching tubular lesions (arrows) in posterior segment of the right upper lobe, representing mucus plugging. Also note endobronchial tumor (arrowhead) in the posterior segmental bronchus of the right upper lobe. Bronchoscopic biopsy disclosed endobronchial metastatic renal cell carcinoma nodule (not shown here). Small centrilobular nodules and branching nodular structures in anterior segment of the right upper lobe are due to concurrent nontuberculous mycobacterial pulmonary disease. (c) High-magnification photomicrograph (×200) of pathologic specimen obtained from the right upper lobe with right upper lobectomy (from a different patient but with same disease) displays endobronchial tumor nodules (arrows). (d) High-magnification photomicrograph (×100) discloses endobronchial tumor nodules (arrows) and distal mucus plugging (open arrows) within the dilated bronchi
Fig. 10.3
Gloved finger sign associated with tuberculous bronchial stricture involving the left lower lobar bronchus in a 67-year-old man who had a history of previous tuberculous infection. (a, b) Mediastinal window and coronal reformatted images (2.0-mm section thickness) of enhanced CT scans obtained at levels of the descending thoracic aorta show branching tubular lesions (arrows) in the left lower lobe, representing mucus plugging. Also note the hypertrophied left bronchial artery and its branches (arrowheads) and destroyed left upper lobe owing to tuberculous infection
Fig. 10.4
Allergic bronchopulmonary aspergillosis in a 64-year-old asthmatic man. (a, b) Lung window images of consecutive CT scans (2.5-mm section thickness) obtained at levels of liver dome show mucus plugging (arrows) in the dilated bronchi in both lower lobes. Also note the dilated bronchi (bronchiectasis) without mucus filling
Fig. 10.5
Allergic bronchopulmonary aspergillosis in a 56-year-old asthmatic woman. (a) Mediastinal window of unenhanced CT scan (2.5-mm section thickness) obtained at level of the right middle lobar bronchus shows high-attenuation V-shaped branching structures (arrows) in lingular division of the left upper lobe. (b) Bronchoscopy depicts yellow mucus (arrows) obstructing lingular divisional bronchus. (c) Low magnification (×8) photomicrograph obtained with bronchoscopic biopsy discloses allergic mucin (mucus plus eosinophils) (arrows) containing calcifications
Table 10.1
Common diseases manifesting as gloved finger sign
Disease | Key points for differential diagnosis |
|---|---|
Benign and malignant neoplasms causing airway obstruction | |
Bronchial atresia | Bronchocele in the apicoposterior segment of the left upper lobe |
Broncholithiasis | Endobronchial or peribronchial location of calcified lymph nodes |
Bronchial tuberculosis | Aneurysmal appearance of medium-sized bronchi |
Foreign-body aspiration | Intrabronchial foreign body with gloved finger sign |
ABPA | Central bronchiectasis with high-attenuation mucus plugging |
Distribution
Congenital bronchial atresia involves the parahilar airways [4]. Broncholithiasis is characterized and associated with peribronchial calcific nodal disease and thus involves usually the segmental bronchi [5]. Aneurysmal appearance of the medium-sized bronchi is seen on CT scans in bronchial tuberculosis [6]. ABPA characteristically involves central airways. Mucus plugging and bronchiectasis usually involve the airways of the upper and middle lung zones in cystic fibrosis.
Clinical Considerations
Almost all patients with ABPA have asthma [7]. In approximately two-thirds of patients with bronchial atresia, the lesions are incidentally found. The remaining patients complain of cough, hemoptysis, fever, and shortness of breath [8]. Hemoptysis is a usual sign in broncholithiasis; it may be massive. Other parenchymal tuberculous lesions usually accompany gloved finger sign in bronchial tuberculosis. Cystic fibrosis is a disease of children, adolescence, and young adults, and most signs and symptoms affect the respiratory or the digestive system.
Key Points for Differential Diagnosis
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


