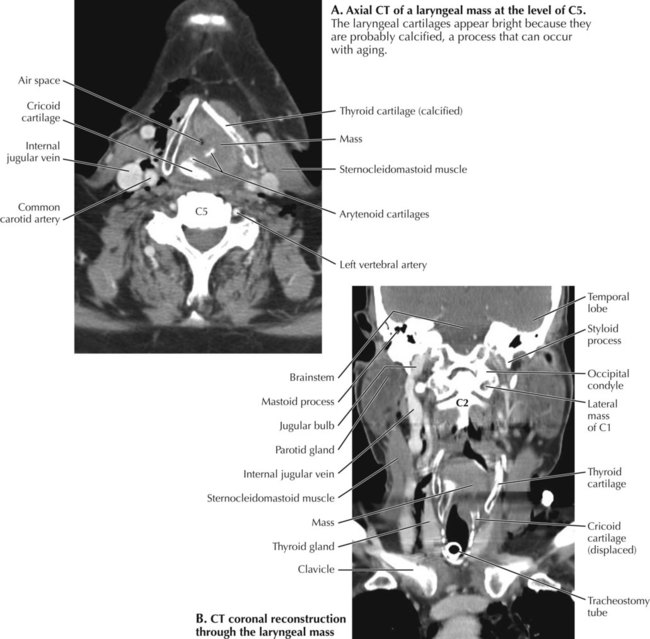
In addition to an analysis of the vertebral compartment (p. 199), a search strategy for the interpretation of neck images includes careful, systematic study of spaces, blood vessels, lymph nodes, organs of the visceral compartment, and other structures and layers visible in the image. A and B are views of a mass in the larynx on the left. In the axial image (A), the thyroid cartilage of the larynx is pushed laterally on the left. The mass is eroding and displacing inferiorly the cricoid cartilage on the left and compromising the air space in the larynx. The coronal view (B) shows an airway tube in the trachea and the mass filling much of the interior of the larynx.
Head and Neck
8.20 Search Strategy: Neck Imaging of Laryngeal Tumor
Radiology Key
Fastest Radiology Insight Engine