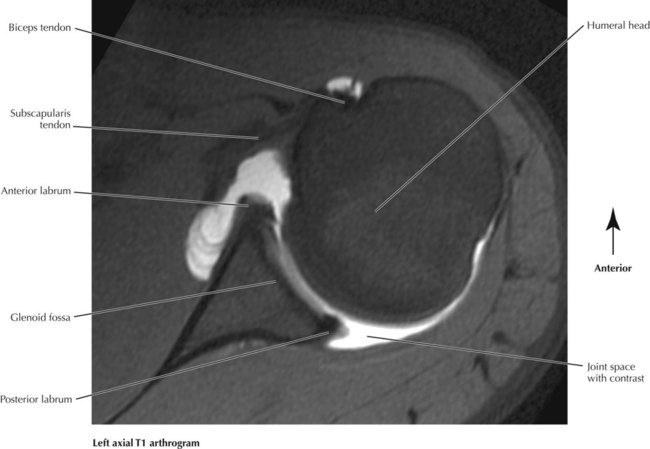
6.2. ANTEROPOSTERIOR SHOULDER X-RAY 6.3. AXILLARY AND Y VIEW X-RAYS OF THE SHOULDER JOINT 6.5. CORONAL T2 MRI OF THE SHOULDER JOINT 6.6. AXIAL T1 ARTHROGRAM OF THE SHOULDER JOINT 6.7. AXILLARY, BRACHIAL, AND ELBOW ARTERIES 6.8. VASCULAR STUDIES OF THE UPPER EXTREMITY 6.10. ARM SERIAL CROSS SECTIONS 6.16. MUSCLES OF THE FOREARM: ANTERIOR VIEW 6.17. MUSCLES OF THE FOREARM: POSTERIOR VIEW 6.18. FOREARM SERIAL CROSS SECTIONS 6.19. UPPER AND MIDDLE FOREARM MRI 6.20. BONES OF THE HAND AND WRIST 6.21. ANTEROPOSTERIOR X-RAY OF THE WRIST AND HAND 6.22. CARPAL BONES AND WRIST JOINT 6.23. T1 AND T2 MRI OF THE WRIST JOINT
Upper Limbs
Radiology Key
Fastest Radiology Insight Engine