• Selected patients treated with posterior decompression with duraplasty
Diagnostic Checklist
• Asymmetric atrophy of lower cervical cord on routine MR in patient with distal upper limb weakness is highly suspicious for Hirayama
Flexion cervical MR recommended
(Left) Sagittal T2WI MR shows the classic appearance of Hirayama disease. The neutral position of the MR shows mild cord atrophy at the C5-C6 level , but is otherwise normal.
(Right) Flexion T2WI MR shows marked ventral displacement of the posterior dural margin with cord compression . A hypointense T2 signal filling the dorsal epidural space is a distended venous plexus, which will homogeneously enhance with contrast (not shown).
(Left) Flexion T1WI MR shows marked ventral displacement of the posterior dural margin with a long segment of cord compression. A slightly heterogeneous signal filling the dorsal epidural space reflects a distended venous plexus .
(Right) Axial T2WI MR in flexion shows a markedly distended posterior epidural plexus . There is ventral displacement of the posterior dura with asymmetrical cord compression, worse on the right .


 , but is otherwise normal.
, but is otherwise normal.
 . A hypointense T2 signal filling the dorsal epidural space is a distended venous plexus, which will homogeneously enhance with contrast (not shown).
. A hypointense T2 signal filling the dorsal epidural space is a distended venous plexus, which will homogeneously enhance with contrast (not shown).
 .
.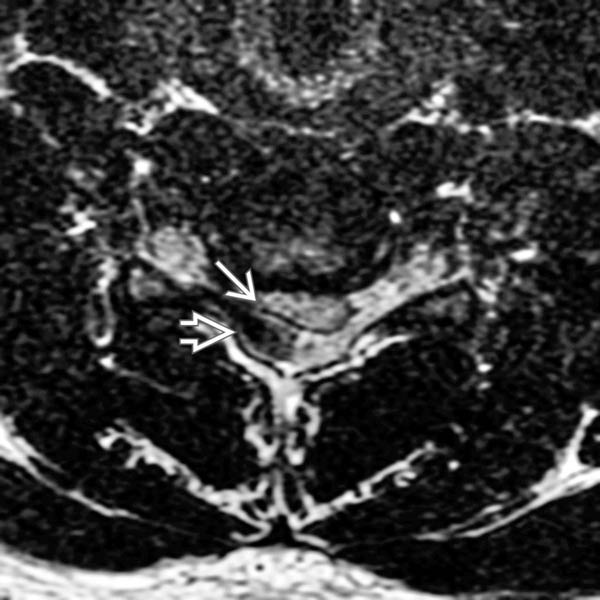
 . There is ventral displacement of the posterior dura with asymmetrical cord compression, worse on the right
. There is ventral displacement of the posterior dura with asymmetrical cord compression, worse on the right  .
.