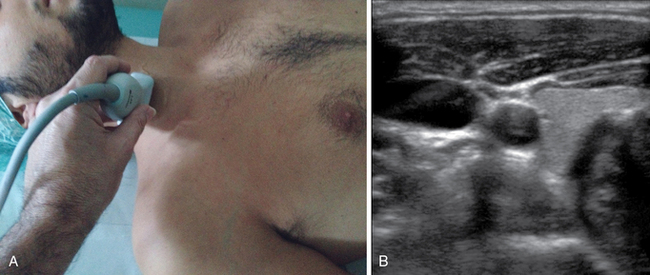
12 Standard central venous access performed with the “blind” technique was historically based on the puncture of two central veins (the subclavian vein and the internal jugular vein),1 but ultrasound (US) guidance has expanded the spectrum to at least four sites: the internal jugular vein, the brachiocephalic (or “innominate”) vein, the subclavian vein, and the axillary vein. In many patients, two additional, centrally located venous segments can be cannulated: the external jugular vein (in its final tract close to the junction of the subclavian vein) and the cephalic vein (in its final, infraclavicular tract close to the junction of the axillary vein). The shift from a “heads-or-tails” choice (subclavian vs. jugular) to a wide spectrum of choices (internal jugular, brachiocephalic, subclavian, axillary, etc.) is the real “Copernican” revolution of the US era. Whereas in the last century the physician was bound to choose between the subclavian and jugular sites on the basis of personal preference, instinct, or experience, selection of the most appropriate vein to cannulate can be determined today on a rational basis by means of US technology.2 US guidance is an evidence-based methodology that significantly reduces the complications related to insertion of CVCs.3–5 However, the benefit of using US is not limited to real-time US-guided venipuncture. The GAVeCeLT (Italian Group for Venous Access Devices) recommended the use of US during CVC insertion for six different purposes: (1) US evaluation of all veins available, (2) choice of the vein on the basis of rational US-based criteria, (3) real-time US-guided venipuncture, (4) US-based control of guidewire/catheter orientation during the procedure, (5) US-based control of pleura-pulmonary integrity after axillary or subclavian vein puncture, and (6) transthoracic echocardiography for verification of the position of the tip of the catheter at the end of the procedure. • The transducer is positioned in a transverse plane at the midneck region (Figure 12-1A). This allows evaluation of the internal jugular vein and carotid artery (short axis; Figure 12-1B). This is an ideal position for an internal jugular vein, US-guided approach using either an “in-plane” or an “out-of-plane” technique. Figure 12-1 First step in the rapid central vein vascular assessment protocol. A,
How to choose the most appropriate ultrasound-guided approach for central line insertion: Introducing the rapid central venous assessment protocol
Overview
The rapid central vein assessment
Related posts:
 Ultrasound-guided peripheral intravenous access
Ultrasound-guided peripheral intravenous access
 Ultrasound-guided arterial catheterization
Ultrasound-guided arterial catheterization
 Ultrasound-guided placement of inferior vena cava filters: (CONSULTANT-LEVEL EXAMINATION)
Ultrasound-guided placement of inferior vena cava filters: (CONSULTANT-LEVEL EXAMINATION)
 Ultrasonography in circulatory failure
Ultrasonography in circulatory failure
 Evaluation of right ventricular function in the intensive care unit by echocardiography: (CONSULTANT-LEVEL EXAMINATION)
Evaluation of right ventricular function in the intensive care unit by echocardiography: (CONSULTANT-LEVEL EXAMINATION)
 Procedural ultrasound for surgeons: (CONSULTANT-LEVEL EXAMINATION)
Procedural ultrasound for surgeons: (CONSULTANT-LEVEL EXAMINATION)
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


How to choose the most appropriate ultrasound-guided approach for central line insertion: Introducing the rapid central venous assessment protocol
