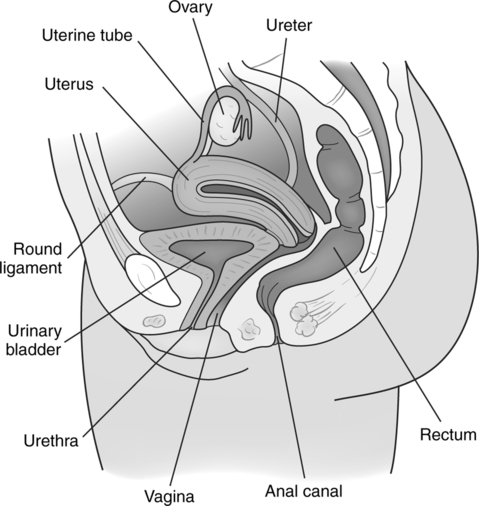
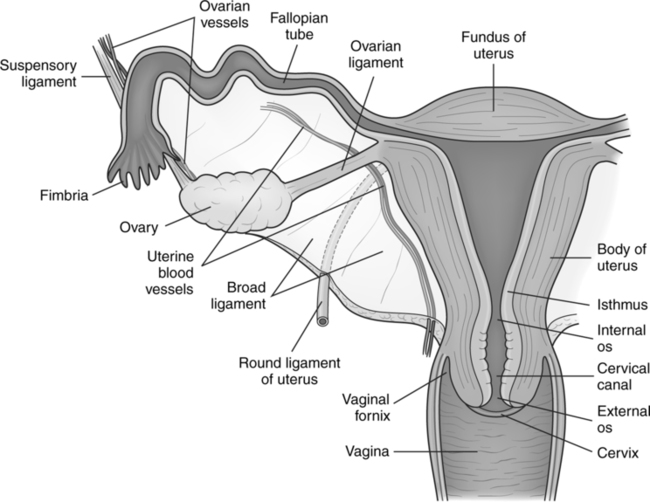
CHAPTER 20 After completing this chapter, the reader will be able to perform the following: Hysterosalpingography involves radiography of the female reproductive system after instillation of a contrast agent. This procedure requires sterile technique, and it is usually performed in a room equipped for specialized genitourinary radiography. Physicians as well as ancillary personnel are required to wear sterile gowns and operating room caps during the procedure. Hysterosalpingography (HSG) is of value in infertility studies and is considered a safe and painless procedure. “Radiation risks from a typical HSG are low, but they may be elevated if fluoroscopic and/or radiographic exposures are prolonged for any reason.”1 The female reproductive organs are divided into external and internal groups. Hysterosalpingography involves mainly the internal group of reproductive organs—the ovaries, uterine tubes, uterus, and vagina (Fig. 20-1). The oviducts can be subdivided into three parts—the isthmus, ampulla, and infundibulum.1 The isthmus is thick-walled and narrow and is attached to the uterine wall. The ampulla is the longest and widest part of the oviduct. Its walls are relatively thin. The funnel-shaped infundibulum terminates in finger-like structures called fimbriae. At this point, the oviduct is opened to the peritoneal cavity. There is, however, one finger of the fimbriae that makes a physical connection with the ovary. The uterus is a thick-walled, muscular organ lying within the pelvis. Its position changes with the degree of fullness of the bladder and rectum. It can also be subdivided into several parts—the fundus, body, isthmus, and cervix (Fig. 20-2). The fundus is the rounded upper portion of the uterus. It is found above the line joining the entrance of the uterine tubes. The body of the uterus, a small triangular area between the uterine walls, extends down toward the isthmus. The body is the main portion of the uterus. Between the cervix and the body of the uterus lies the isthmus, a narrow, constricted, very short segment about 1 cm long. The cervix communicates with the vagina, and can be divided into a supravaginal and a vaginal part. The vaginal portion extends into the vagina, whereas the supravaginal part extends up to the isthmus. The contrast agents used to delineate anatomic structures during hysterosalpingography are divided into two groups—water-soluble and oily. All are organic iodine compounds, and each group has its advantages. The water-soluble contrast agents are absorbed quickly and do not leave a residue within the genital tract2; the ethiodized oils are extremely opaque and are well tolerated by the structures under study. The low-osmolality contrast agents offer a reduction in the burning sensation and pain experienced with the ionic water-soluble contrast agents. The choice of contrast agent is governed by physician preference and institutional protocol. The oily contrast agents are almost never used today because the water-soluble organic iodides have proved their effectiveness for this procedure. Reference to the oily contrast agents is included because they are still manufactured and occasionally used. Table 20-1 is a comparison of oily contrast media with water-soluble media. TABLE 20-1 Comparison of Oily and Water-Soluble Contrast Media
Hysterosalpingography
 Identify the anatomy of the female reproductive system
Identify the anatomy of the female reproductive system
 List the indications and contraindications for the procedure
List the indications and contraindications for the procedure
 Identify the type of contrast media used for the procedure
Identify the type of contrast media used for the procedure
 Describe the patient preparation for the procedure
Describe the patient preparation for the procedure
 List the specialized equipment necessary for the procedure
List the specialized equipment necessary for the procedure
 Describe the patient positioning for the procedure
Describe the patient positioning for the procedure
 Explain the other modalities used to evaluate the female reproductive system
Explain the other modalities used to evaluate the female reproductive system
ANATOMIC CONSIDERATIONS
Uterine Tubes
Uterus
CONTRAST AGENTS
Characteristic
Oil-Based Contrast Media*
Water-Soluble Media
Viscosity
High
Low to moderate
Radiopacity
Very good
Moderate to satisfactory
Absorption rate
Very slow; delayed for many months when large amounts are injected
Prompt excretion through kidneys after 20–60 minutes; this can be a desirable trait
In cases of hydrosalpinx, absorption is slower; contrast may persist for 24–48 hours
Toxicity
Not observed unless decomposed oil is used.
Rare
Allergic reactions
Not observed
Occasionally observed
Peritoneal reactions
Only when large amounts are injected; not observed when small amounts are used
Observed, mostly transient
Pain
Not observed when small amounts are injected under low pressure; few complaints when pressures <200 mm Hg are used
Nearly always present; may be transient or persist for several hours post procedure
Dangers
Intravasation, pulmonary embolism
Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree

 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access