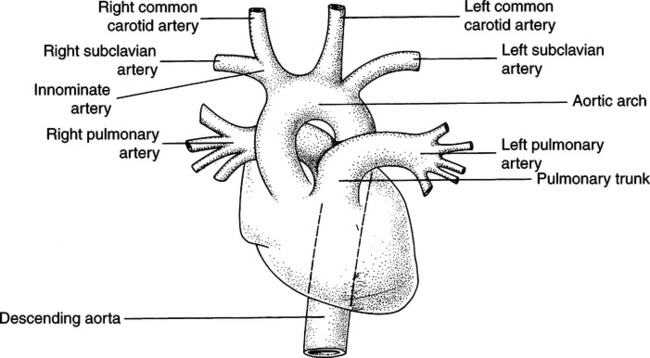
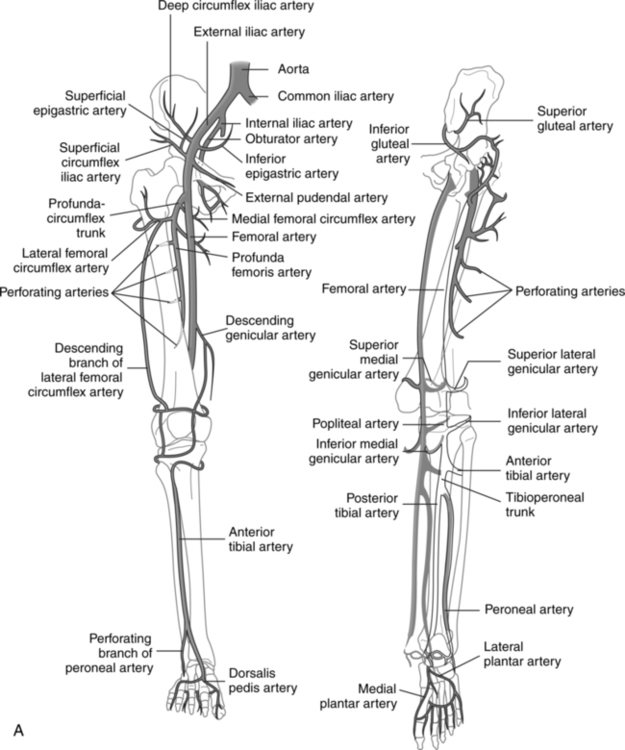
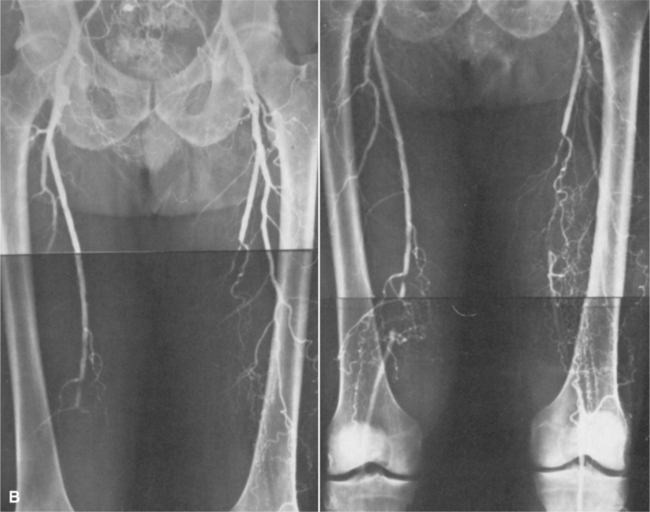
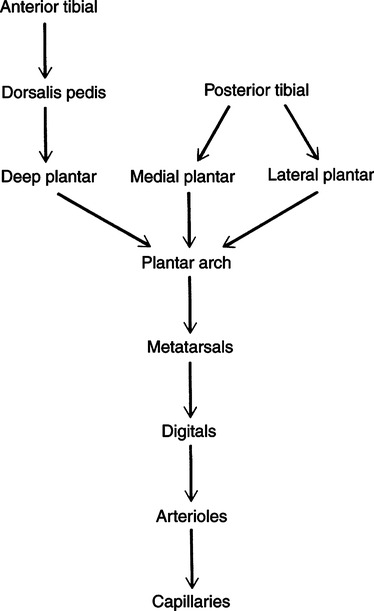
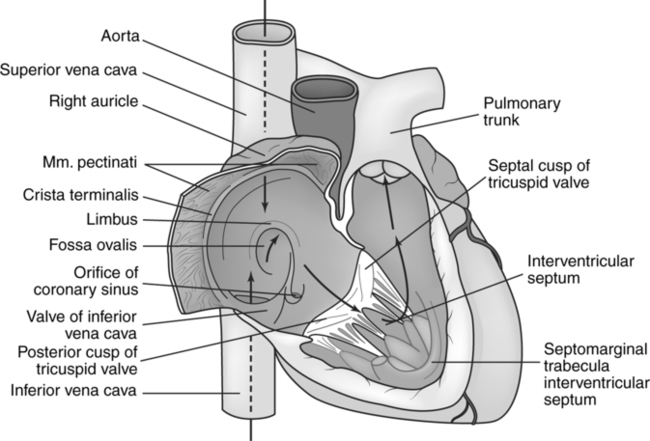
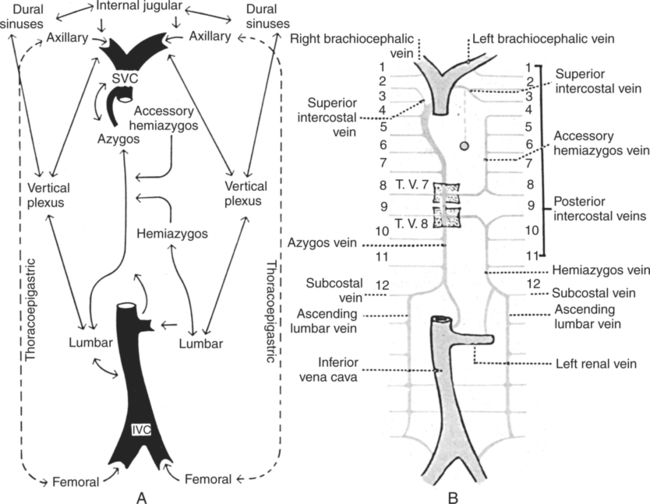
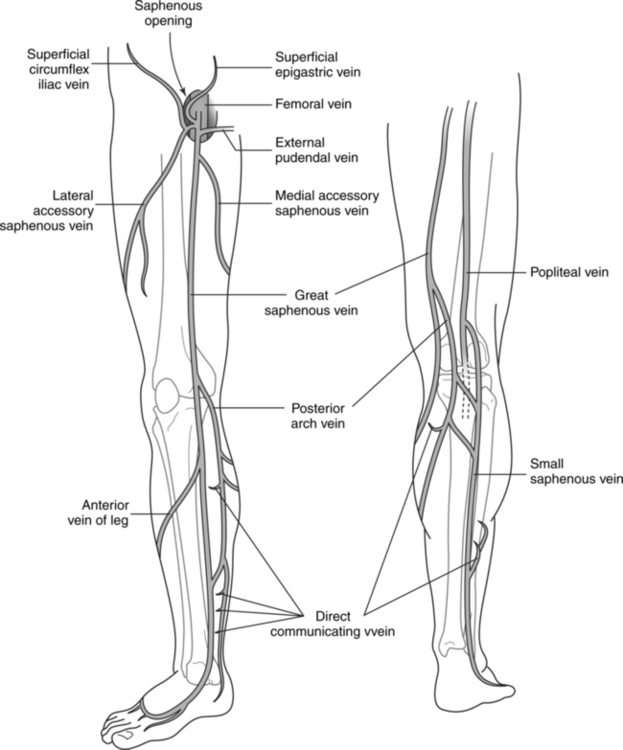
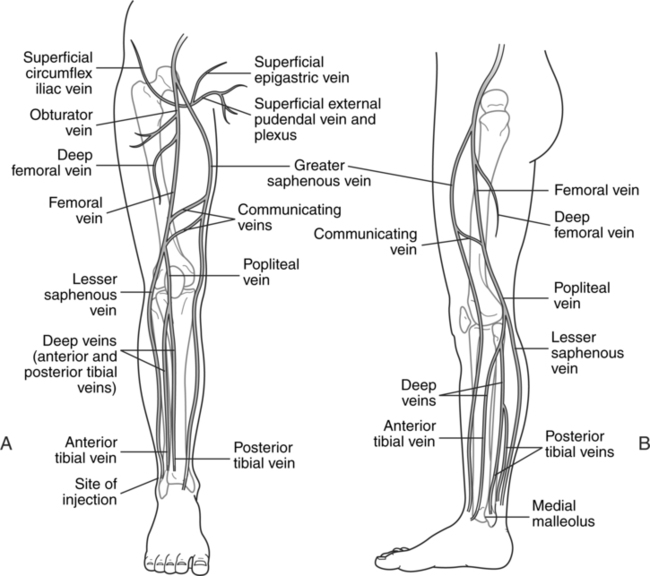
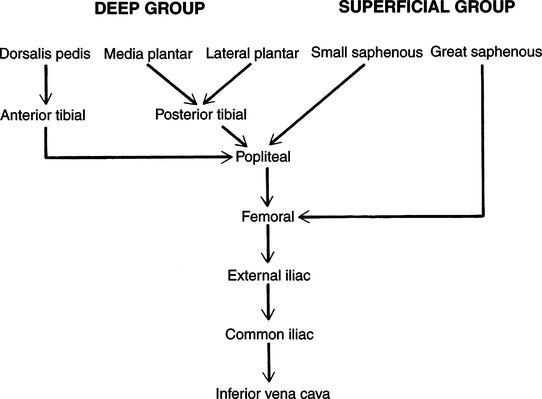
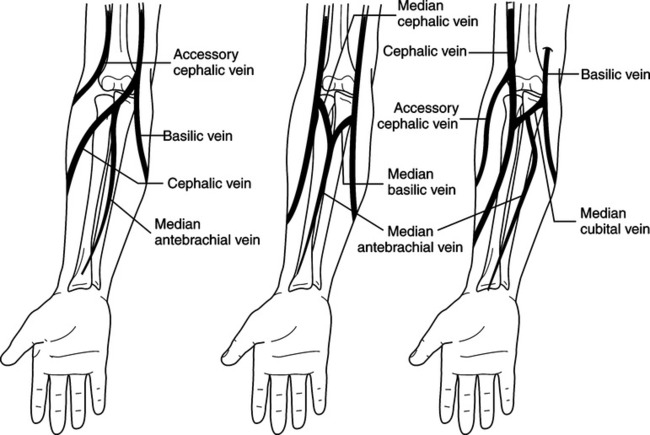
CHAPTER 15 After completing this chapter, the reader will be able to perform the following: The aortic arch gives off three major vessels: the brachiocephalic, left common carotid, and left subclavian arteries (Fig. 15-1). The brachiocephalic artery is the first major branch coming off the aorta. It splits into the right subclavian and the right common carotid arteries. The vertebral artery courses up to enter the skull. This vessel supplies the deep structures in the neck. It also gives off branches referred to as the spinal arteries to supply the spinal cord and the meninges. It then courses into the skull where it joins the basilar artery. The anatomy of the vertebral artery will be discussed in depth in Chapter 16. The internal iliac arteries supply blood to the pelvic region, whereas the external iliac arteries are the origin of the blood supply to the lower extremities (Fig. 15-2,A and B). The external iliac artery courses for about 10 cm before becoming the femoral artery at a point midway between the anterior superior iliac spine and the symphysis pubis. This is also the level at which the femoral artery enters the lower extremity. The branches of the femoral artery are divided into superficial and deep branches, as summarized in Box 15-1. The posterior tibial artery is a direct continuation of the popliteal artery. Coursing downward toward the ankle, it passes between the medial malleolus of the tibia and the calcaneus and terminates in the foot. As in the anatomy of the anterior tibial artery, the major branches of the posterior tibial artery—the peroneal, nutrient, communicating, posterior medial malleolar, and medial calcaneal arteries—are concentrated around the knee and ankle joints. A summary of the circulation from the level of the anterior and posterior tibial arteries is given in Figure 15-3. The veins of the body collect the blood from the systemic circulation and return it to the heart and lungs for reoxygenation. The venous system of the body is extensive, and consideration is given here only to major veins with significance in venous angiography. The venous system of the body ultimately empties into two major veins—the inferior and superior venae cavae—which direct the venous blood into the right atrium of the heart (Fig. 15-4). All of the major veins are tributaries of these vessels and compose the venous circulation. The superior vena cava receives blood from the upper portion of the body, and the inferior vena cava serves the lower portion. There are two major superficial veins of the upper extremity—the cephalic vein and the basilic vein of the forearm (Fig. 15-5). These vessels are the primary means of drainage in the upper extremity. The cephalic vein starts in the distal forearm, receives the drainage from the dorsal aspect of the hand, runs along the lateral aspect of the arm, and ends just below the clavicle. At this point, the vein courses medially and joins the axillary vein. The median cubital vein forms a connection between the cephalic and the basilic veins of the upper extremity and is located on the anterior aspect of the arm at the level of the elbow. This vein is the usual location for blood sampling, intravenous injection, blood transfusion, and introducing catheters for contrast radiography. The basilic vein runs up from the distal forearm toward the medial side of the arm, where it ultimately becomes the axillary vein. The median vein collects the venous return from the palmar aspect of the hand. It then courses over the anterior of the arm until it joins the basilic vein. In another variant of the normal anatomy, the median vein can also join the median cubital vein. The axillary vein continues a short distance and becomes the subclavian vein at approximately the level of the first rib. The subclavian vein is then joined by the internal jugular vein to form the brachiocephalic vein. The brachiocephalic vein also collects blood from the vertebral, internal mammary, intercostal, and thyroid veins. The azygos and hemiazygos system comprises unpaired vessels that lie on each side of the spine (Fig. 15-6). There are several normal variants of the anatomic presentation of this system of veins. The superficial veins are represented primarily by the great and small saphenous veins. The accessory saphenous vein also contributes to the return of blood from the lower extremity, when it is present. It is usually located over the posteromedial aspect of the thigh and communicates with both the great and small saphenous veins. The great saphenous vein originates at the medial side of the foot at the level of the median marginal vein. It continues in front of the medial malleolus, ascends along the anteromedial aspect of the lower leg and thigh, and ends in the common femoral vein. The location of this vessel at the medial malleolus provides an excellent avenue for intravenous administration of medications, if necessary. The small saphenous vein, also called the lesser saphenous vein, originates on the lateral side of the foot at the level of the lateral marginal vein. It then courses toward the posterior of the lower leg and ascends to above the knee joint. Several normal variants may be present at this level, and the small saphenous vein joins the popliteal, greater saphenous, or deep muscular calf veins (Fig. 15-7). The deep veins of the lower extremity consist primarily of the femoral and popliteal. These are usually paired and accompany the arteries. These normally originate with the vessels in the plantar surface of the foot and follow the course of the anterior tibial, posterior tibial, and peroneal arteries. The anterior and posterior tibial veins ascend to just below the level of the knee, where they anastomose to form the popliteal vein (Fig. 15-8). At approximately the level of midthigh, the popliteal veins become the superficial femoral vein. This vein ascends until it is joined by the deep femoral vein. This occurs about 5 to 10 cm below the inguinal ligament; the resultant vessel is called the common femoral vein. The common femoral vein becomes the external iliac vein above the inguinal ligament. It connects with the internal iliac vein to become the common iliac vein. At about the level of the fifth lumbar vertebra, the left and right iliac veins join to become the inferior vena cava. A summary of the venous circulation of the lower extremity is given in Figure 15-9. Table 15-1 summarizes the branches that arise from the external and internal iliac arteries. TABLE 15-1 Summary of Branches from the External and Internal Iliac Arteries
Peripheral Vascular Procedures
 Discuss the vascular anatomy of the upper and lower extremities and the pelvis
Discuss the vascular anatomy of the upper and lower extremities and the pelvis
 List the various procedures that can be performed in these areas
List the various procedures that can be performed in these areas
 List the indications and contraindications for angiography in these areas
List the indications and contraindications for angiography in these areas
 Discuss vessel access for these procedures
Discuss vessel access for these procedures
 List the contrast agents that are suggested for peripheral angiography
List the contrast agents that are suggested for peripheral angiography
 Discuss the patient positioning for peripheral angiography
Discuss the patient positioning for peripheral angiography
ANATOMIC CONSIDERATIONS
Arterial Supply
Upper Extremity
Lower Extremity
Veins
Upper Extremity
Lower Extremity
Pelvic Circulation
Artery
Branch
Sub Branches
External iliac
Inferior epigastric artery
Deep iliac circumflex
Internal iliac
Anterior trunk
Superior vesical
Inferior vesical
Middle hemorrhoidal
Obturator
Internal pudendal
Uterine
Prostatic
Inferior gluteal
Posterior trunk
Iliolumbar
Lateral sacral superior gluteal Related posts:
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Peripheral Vascular Procedures