Iatrogenic Lung Diseases: Drug-Induced Lung Disease and Radiation Pneumonitis
Iatrogenic Lung Diseases: Drug-Induced Lung Disease and Radiation Pneumonitis
W. Richard Webb
DRUG-INDUCED LUNG DISEASE
Many drugs, both therapeutic and illicit, can be associated with lung disease. However, drug-induced lung disease is manifested in a limited number of ways. Specific pathologic reactions occurring with pulmonary drug toxicity include the following:
Hydrostatic and increased permeability pulmonary edema
Diffuse alveolar damage (DAD) and the acute respiratory distress syndrome (ARDS)
Pulmonary hemorrhage
Organizing pneumonia (OP/BOOP)
Eosinophilic pneumonia and hypersensitivity reactions
Chronic interstitial pneumonitis with fibrosis
Systemic lupus erythematosus (SLE)
Pulmonary vasculitis and pulmonary hypertension
Bronchiolitis obliterans
Each of these patterns is characteristically associated with a different group of drugs, although many drugs can result in more than one type of lung reaction, and some overlap between these patterns is common. In most cases, the radiographic appearances of a drug-related lung disease are nonspecific and the diagnosis must be based on observing a temporal relationship between the administration of a drug and the development of pulmonary abnormalities.
Because of the large number of drugs associated with drug reactions and the variety of patterns possible, a high degree of suspicion must be maintained when evaluating patients with unexplained lung disease, regardless of what it looks like or what drug treatment is being employed. Prompt recognition of drug-induced lung disease is important because early abnormalities may resolve completely if the drug is discontinued or appropriate therapy is instituted.
Radiographic abnormalities associated with drug-related lung injury vary with the histologic pattern present, and with a few exceptions, the appearance of each pattern appears the same regardless of the drug involved. High-resolution CT (HRCT) is more sensitive than chest radiography in defining the radiographic abnormalities.
Pulmonary Edema
Hydrostatic pulmonary edema may result from drugs affecting the heart or systemic vasculature (Table 17-1). An example would be cocaine. Radiographic and HRCT findings are typical of any cause of hydrostatic edema. Pleural effusion may be present.
Increased permeability pulmonary edema also may occur. Onset is usually sudden. Increased permeability pulmonary edema occurring without DAD results in typical findings of pulmonary edema, including interlobular septal thickening (Kerley’s lines; see Fig. 11-11 in Chapter 11), ground-glass opacity (see Fig. 11-13 in Chapter 11), and to a lesser extent, consolidation. This occurrence is typical of interleukin-2, but many other drugs are capable of causing increased permeability pulmonary edema. These include aspirin, nitrofurantoin, heroin, and cytotoxic agents such as methotrexate, cyclophosphamide, and BCNU. Unlike with hydrostatic edema, pleural effusion is typically absent. Prompt resolution may occur with appropriate treatment.
TABLE 17.1 Drugs Associated with Pulmonary Edema
Aspirin and salicylates
BCNU
Cocaine
Chlordiazepoxide
Codeine
Cyclophosphamide
Cytosine arabinoside
Heroin
Hydrochlorothiazide
Interleukin-2
Lidocaine
Methadone
Methotrexate
Nitrofurantoin
Nonsteroidal anti-inflammatory drugs
OKT3
Propoxyphene
Tocolytics (ritodrine and terbutaline)
Trimethoprim-sulfamethoxazole
Tricyclic antidepressants
Diffuse Alveolar Damage
DAD with ARDS can be caused by a variety of drugs, most typically cytotoxic agents (e.g., bleomycin, busulfan, and cyclophosphamide), nitrofurantoin, and amiodarone (Table 17-2). As with pulmonary edema, onset is usually sudden and occurs within a few days of the onset of chemotherapy.
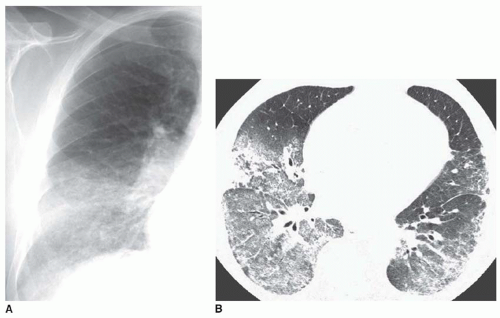
DAD reflects a more serious lung and capillary endothelial injury than occurs with increased permeability pulmonary edema. The acute or exudative stage of DAD occurs in the first week after injury and is characterized by necrosis of alveolar pneumocytes, edema, hemorrhage, and hyaline membrane formation. Radiographs and CT typically show extensive bilateral parenchymal consolidation, usually most marked in the dependent lung regions; interlobular septal thickening and Kerley’s lines are typically absent (Fig. 17-1). Other than a temporal relationship to chemotherapy, there are no clinical or CT findings that allow this appearance to be distinguished from other causes of ARDS. The reparative stage of DAD, characterized by cellular hyperplasia and fibrosis, occurs after 1 to 2 weeks. Depending on the severity of the lung injury, abnormalities may regress, stabilize, or progress to fibrosis and honeycombing.
FIG. 17.1. Diffuse alveolar damage resulting from treatment with doxorubicin (Adriamycin). A: Chest radiograph coned to the right lung shows basilar consolidation. B: HRCT shows ground-glass opacity and consolidation with a basal and dependent predominance.
TABLE 17.2 Drugs Associated with Diffuse Alveolar Damage
Amiodarone
BCNU
Bleomycin
Busulfan
Chlorambucil
Cyclophosphamide
Cytosine arabinoside
Gold
Methotrexate
Mitomycin
Melphalan
Nitrofurantoin
Oxygen
Penicillamine
Tricyclic antidepressants
Vinblastine and vinca alkaloids
Pulmonary Hemorrhage
Drug-related diffuse pulmonary hemorrhage is uncommon. Typical causes include anticoagulants, cyclophosphamide, and penicillamine. Hemoptysis may or may not be present (Table 17-3). Radiographic and HRCT findings are typical of pulmonary hemorrhage, with bilateral patchy ground-glass opacity or consolidation (see Chapter 19). Pleural effusion is typically absent.
TABLE 17.3 Drugs Associated with Pulmonary Hemorrhage
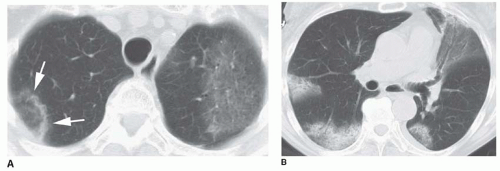
Organizing pneumonia/bronchiolitis obliterans organizing pneumonia (OP/BOOP) has been described with methotrexate, gold, penicillamine, nitrofurantoin, amiodarone, bleomycin, and busulfan (Table 17-4). Symptoms include progressive cough, dyspnea, and fever. Like other causes of OP/BOOP (see Chapter 13), this pattern is characterized by consolidation or ground-glass opacity that may have a patchy or nodular distribution and may predominate in a peribronchial or subpleural location (Figs. 17-2 and 17-3). Lung nodules with or without the “atoll sign” or “reversed halo sign” may be present (Figs. 17-2A and 17-3). OP/BOOP tends to predominate in the lower lobes (see Fig. 17-3).
Hypersensitivity Reactions and Eosinophilic Pneumonia
Hypersensitivity reactions can be attributed to a large number of drugs but are most commonly due to methotrexate, nitrofurantoin, bleomycin, procarbazine, BCNU, cyclophosphamide, nonsteroidal anti-inflammatory drugs, and sulfonamides; their presence is unrelated to the cumulative drug dose (Table 17-5).
FIG. 17.2. Organizing pneumonia/bronchiolitis obliterans organizing pneumonia (OP/BOOP) occurring in association with chemotherapy for breast carcinoma. A. CT through the lung apex shows ground-glass opacity in the left upper lobe and a ring of ground-glass opacity in the right upper lobe (arrows), representing the atoll sign of OP/BOOP. B: CT shows patchy subpleural areas of consolidation and ground-glass opacity typical of OP/BOOP.
TABLE 17.4 Drugs Associated with Organizing Pneumonia/Bronchiolitis Obliterans Organizing Pneumonia
Amiodarone
Bleomycin
Busulfan
Cyclophosphamide
Gold
Interferon
Methotrexate
Nitrofurantoin
Penicillamine
Sulfasalazine
Hypersensitivity reactions may have features of simple eosinophilia (Loeffler’s syndrome), chronic eosinophilic pneumonia, or acute eosinophilic pneumonia. Cough and dyspnea, with or without fever, can be acute in onset or progress over a period of several months following institution of treatment. A peripheral eosinophilia is present in up to 40%. These reactions are characterized on chest radiographs and HRCT by patchy areas of consolidation or ground-glass opacity, which may be chronic or relatively acute, transient, and fleeting. A peripheral and subpleural distribution may be seen.
Chronic Interstitial Pneumonitis and Fibrosis
Both usual interstitial pneumonia (UIP) and nonspecific interstitial pneumonia (NSIP) have been associated with drug injury; in some cases the pattern may overlap that of OP/BOOP or DAD. The clinical and radiographic presentations are often identical to those of idiopathic pulmonary fibrosis. A long list of drugs has been implicated in the development of chronic pneumonitis, but this pattern is most commonly the result of cytotoxic chemotherapeutic agents such as bleomycin, busulfan, methotrexate, doxorubicin, and carmustine (BCNU; Table 17-6). Nitrofurantoin, amiodarone, gold, and penicillamine are noncytotoxic drugs that can also result in this type of reaction.
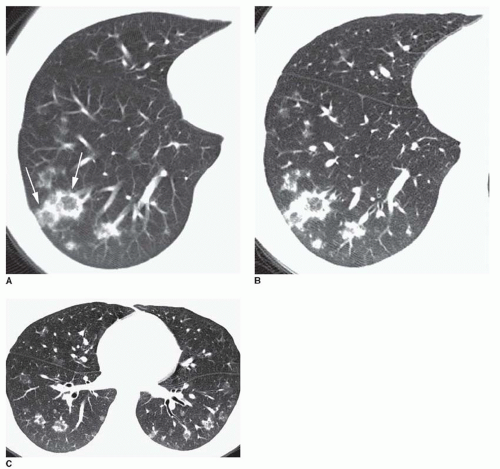
FIG. 17.3. Nodular organizing pneumonia/bronchiolitis obliterans organizing pneumonia related to chemotherapy for Ewing’s sarcoma. A: CT through the right lower lobe shows scattered nodules. Some have a dense rim and a ground-glass opacity center, the so-called atoll sign (arrows). B: HRCT at the same level. C: HRCT at a different level shows bilateral nodules of soft-tissue attenuation and groundglass opacity visible in both lower lobes. Some nodules show the atoll sign.
TABLE 17.5 Drugs Associated with Eosinophilic Pneumonia and Hypersensitivity Reactions
BCNU
Bleomycin
Cyclophosphamide
Diphenylhydantoin
Erythromycin
Ethambutol
Fluoxetine
Gold
Imipramine
Isoniazid
Methotrexate
Nitrofurantoin
Nonsteroidal anti-inflammatory drugs
Paraaminosalicylic acid
Penicillamine
Penicillin
Procarbazine
Sulfasalazine
Tetracycline
Plain radiographs in patients with chronic pneumonitis and fibrosis typically show a mixture of reticulation and consolidation; abnormalities are usually bilateral and symmetric, with a predominant lower lung zone involvement.
The most common pattern seen on HRCT in patients with chronic pneumonitis and fibrosis includes irregular reticular opacities (Fig. 17-4), honeycombing (Fig. 17-5), architectural distortion, and traction bronchiectasis, with or without associated consolidation; ground-glass opacity may be seen in early cases (see Figs. 17-4,17-5,17-6,17-7 and 17-8). As on chest radiographs, HRCT abnormalities are usually bilateral and symmetric, with a predominant lower lung zone involvement. A peripheral and subpleural distribution of abnormalities is common, particularly in patients with bleomycin toxicity. Patchy fibrosis may be seen in patients receiving nitrofurantoin. The extent of abnormalities depends on the severity of lung damage. Mild damage is often limited to the posterior subpleural lung regions of the lower lung zones. In patients with more severe abnormalities, there is greater involvement of the remaining lung parenchyma.
Only gold members can continue reading. Log In or Register to continue
Oct 10, 2016 | Posted by drzezo in CARDIOVASCULAR IMAGING | Comments Off on Iatrogenic Lung Diseases: Drug-Induced Lung Disease and Radiation Pneumonitis