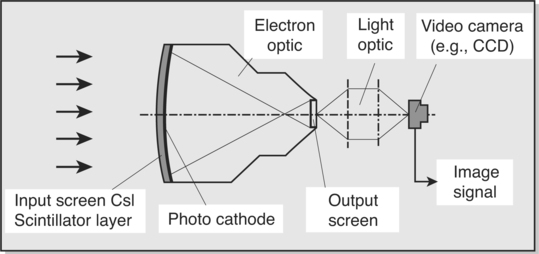
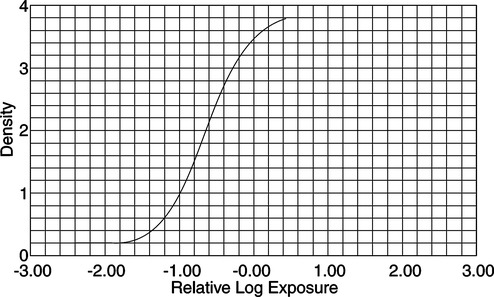
CHAPTER 2 After completing this chapter, the reader will be able to perform the following: 1. Film changer and mounting stand assembly. This was the drive portion of the roll film changer. It housed the mechanism necessary to transport the film from the supply magazine to the receiving magazine. 2. Supply magazine. This served to hold the unexposed roll of film. 3. Receiving magazine. This could be transported to the darkroom under normal lighting conditions without the risk of exposure of the film by light. 4. Program selector. This was the heart of the variable speed film changers. It operated the film changer during single or serial exposures and established the film rate (number of films per second) and the duration of each phase. All of the rapid serial changers discussed operated in a similar manner (Fig. 2-1). They moved the imaging material into place for the exposure and then removed it to a storage location. In other words, with all rapid serial changers there was a period of time during which the film or cassette was in motion (transport time) and a period of time during which no motion occurred and the film was in position for the exposure (stationary period). The radiograph had to be produced during the stationary period. The stationary period for each of the types of rapid serial changers was different; however, it was usually less than 50% of the total film cycle time (transport time + stationary period). Certain inherent electronic delays prevented the entire stationary period from being used to make the exposure. These were the zero time and phase-in time. The actual amount of phase-in time varied with each exposure and could not be predetermined. However, the maximum exposure time that could be used for a particular system was calculated by deducting the greatest phase-in time delay from the stationary period. Table 2-1 illustrates the maximum phase-in time delays for single-phase and three-phase units. TABLE 2-1 An image intensifier (II) is used to increase the brightness of the image. This is accomplished with the II tube (Fig. 2-3). The input side of the II tube is coated with a phosphor layer, usually cesium iodide, that produces the image as a direct result of the action of the remnant radiation. Photoemissive material is coated on the substrate opposite the phosphor layer; this material converts the visible light image into an electron image. The electrons making up the image are accelerated across the II tube by an electron lens system and focused to strike the output side of the tube. The American College of Radiology (ACR) and the National Electronics Manufacturers Association (NEMA) recognized this with the advent of computed tomography and formed a consortium to develop a standard for file formats that could be understood by equipment and systems manufactured by different companies. The format was termed the Digital Imaging and Communications in Medicine Standard, or DICOM. In 1983 the ACR and NEMA formulated a standard1 that would: The original standard was published in 1985, and it proposed a specific type of interface, special software commands, and consistent data formats. Since the original standard was published, it has undergone several revisions that include several enhancements to the original version. NEMA views the DICOM standard as an evolving set of guidelines. The DICOM standard is directed at providing a platform for the interoperability of various devices and systems primarily in the area of diagnostic medical imaging. The specific guidelines and specifications of the DICOM standard are beyond the scope of this text. They are available from the National Electrical Manufacturers Association and can be found on their website—(http://www.nema.org). Previously, magnetic videodisc systems were used to indirectly record the images produced during the study using a rigid disc coated with an emulsion similar to magnetic tape. These have been replaced by recordable CD-ROM devices that use the CD Medical DICOM 3 international format. An example of this type of system is the Siemens ACOM, an archiving and review station with accompanying ACOM.PC software (Fig. 2-4). The computer system is a relatively small computer system, which houses the DICOM software. The information from this system can be sent to a PACS workstation, or the images can be archived either on the hard drive or on CD-ROM. Initial systems used various methods to produce the images. These included motorized optics and multiple lenses to produce the images. By varying the distances of the lenses and the film, it became possible to change the size of the images produced. Many advances were introduced to improve on the quality of the output produced by these cameras. These included better optics, the use of flat screen monitors. and improved phosphors. Eastman Kodak produces several types of single-emulsion radiographic film for use with the multiformat camera. Figure 2-5 illustrates the sensitometric properties of three of Eastman Kodak’s multiformat films. Note that there is a suitable variety of film speeds and average gradients among the films. These are all sensitive to the higher wavelength green light and are compatible with most CRT monitors. These cameras are still employed in many institutions and find their greatest use in ultrasound and nuclear medicine.
Image Capture—Analog and Digital
 Describe the history of image recording in advanced procedures
Describe the history of image recording in advanced procedures
 Define the roll and cut film changers from a historical perspective
Define the roll and cut film changers from a historical perspective
 Identify the various indirect methods of recording the radiographic images
Identify the various indirect methods of recording the radiographic images
 Define the basic concepts of analog versus digital imaging
Define the basic concepts of analog versus digital imaging
 Identify the use of flat panel detector systems
Identify the use of flat panel detector systems
 List and describe the principles underlying radiographic subtraction
List and describe the principles underlying radiographic subtraction
DIRECT IMAGING SYSTEMS
Rapid Serial Film Changers—An Historical Perspective
Roll Film Changers
Basic Operational Considerations
 Zero time was the delay caused by the operational time of the relays and contacts in the x-ray exposure control. This delay was constant for any particular apparatus and was preset by the manufacturer
Zero time was the delay caused by the operational time of the relays and contacts in the x-ray exposure control. This delay was constant for any particular apparatus and was preset by the manufacturer
Type of Unit
Maximum Phase-in Time (s)
Calculation of Maximum Phase-in Time*
Maximum Phase-in Time (ms)
Single Phase
1/60
1000/60
16.67
Three Phase
1/360
1000/360
2.78

INDIRECT IMAGING SYSTEMS
Image Intensification
IMAGE OUTPUT
DICOM Standard
 Promote the communication of digital imaging information, regardless of the manufacturer of the device
Promote the communication of digital imaging information, regardless of the manufacturer of the device

Hard Copy Image Output
Photofluorographic Systems
Multiformat Cameras.
Radiology Key
Fastest Radiology Insight Engine







 s and for three-phase units,
s and for three-phase units,  s.
s.