 arising from the superior mesenteric artery. The left gastric artery also has a separate origin from the aorta, though difficult to perceive on this image. The “celiac trunk” in this patient consists only of the splenic artery. Congenital variations of vascular anatomy are very common.
arising from the superior mesenteric artery. The left gastric artery also has a separate origin from the aorta, though difficult to perceive on this image. The “celiac trunk” in this patient consists only of the splenic artery. Congenital variations of vascular anatomy are very common.

 from the superior mesenteric artery.
from the superior mesenteric artery.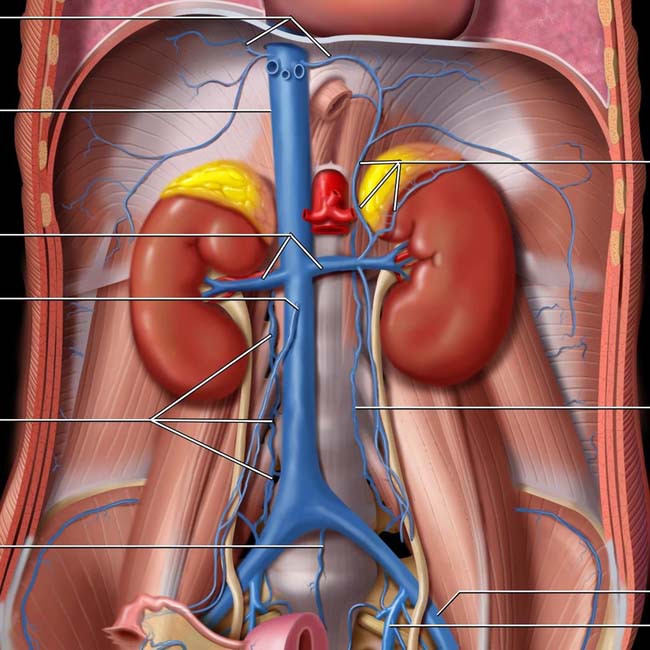
Inferior vena cava (IVC)
Renal veins
Right gonadal vein
Ascending lumbar vein
Middle sacral vein
Adrenal veins
Ascending lumbar vein
External iliac vein
Internal iliac (hypogastric) vein
(Top) The inferior vena cava (IVC) is formed by the confluence of the common iliac veins, which are formed by the confluence of the internal and external iliac veins. Note the ascending lumbar veins, which anastomose freely between the IVC and azygous, hemiazygos, and renal veins. These form a pathway for collateral flow in the event of IVC obstruction and play an important role in the systemic spread of pelvic tumors and infection.
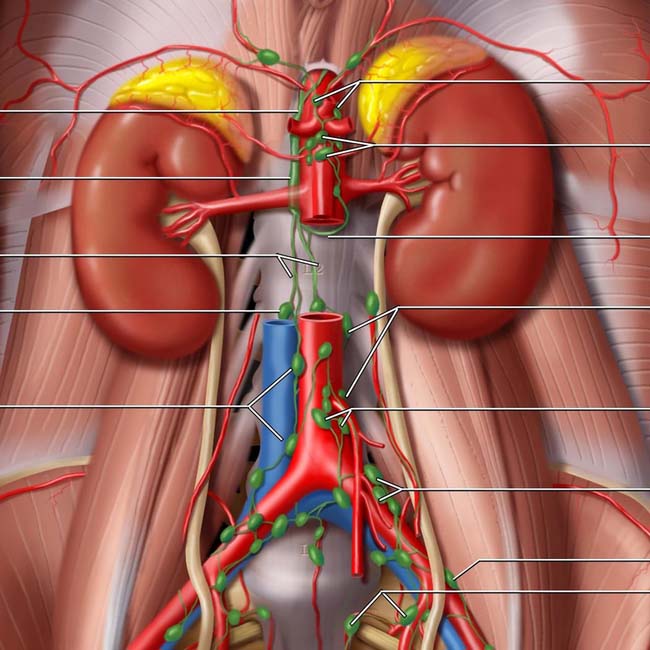
Cisterna chyli
Lumbar trunks (of cisterna chyli)
Right lumbar (retrocaval) node
Aortocaval nodes
Celiac nodes
Superior mesenteric nodes
Intestinal trunk (of cisterna chyli)
Lumbar (paraaortic) nodes
Inferior mesenteric nodes
Common iliac nodes
External iliac node
Internal iliac (hypogastric) nodes
(Bottom) The major lymphatics and lymph nodes of the abdomen are located along, and share the same name as, the major blood vessels.

 and retrocrural
and retrocrural  lymph nodes.
lymph nodes.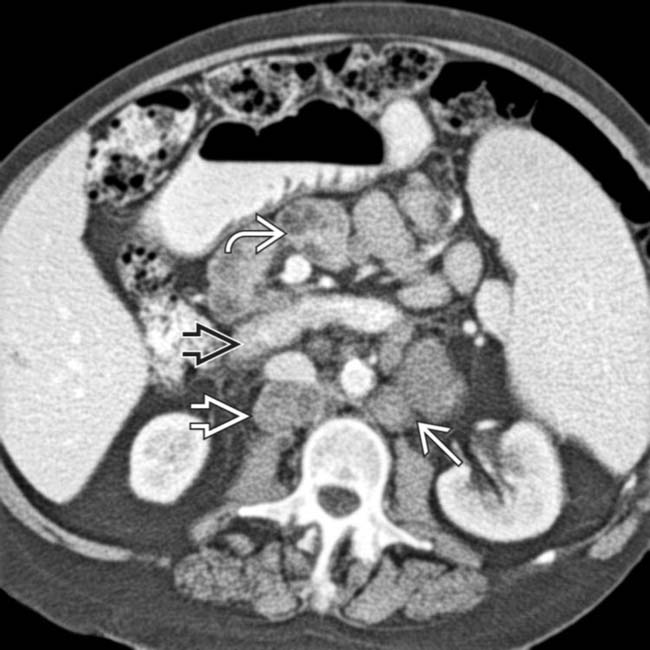
 is displaced by large retroperitoneal nodes; the mesenteric vessels are surrounded or “sandwiched” by mesenteric nodes
is displaced by large retroperitoneal nodes; the mesenteric vessels are surrounded or “sandwiched” by mesenteric nodes  . The lumbar nodes are often referred to as para- or retroaortic
. The lumbar nodes are often referred to as para- or retroaortic  (or -caval)
(or -caval)  , indicating their position relative to the great vessels.
, indicating their position relative to the great vessels.
 .
.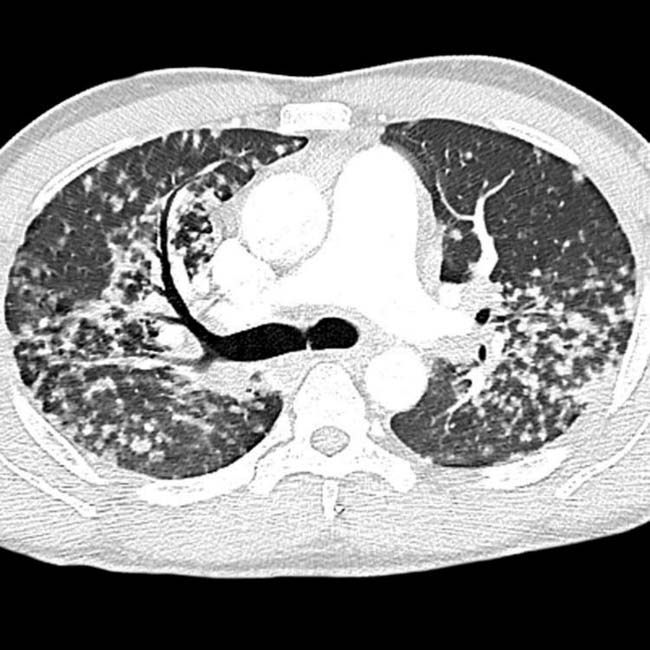

 in both kidneys, as well as upper abdominal lymphadenopathy
in both kidneys, as well as upper abdominal lymphadenopathy  .
.Related posts:
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


