Fig. 19.1
Normal orbital and ocular anatomy. (a) Plain radiograph (Water’s view) demonstrates osseous anatomy. The superior orbital fissure (2) separates the roof from the lateral wall of the orbit. The lateral wall of the orbit is constituted by the greater wing of the sphenoid (4). The roof is constituted by the orbital plate of the frontal bone (5) and lesser wing of the sphenoid (3). The optic canal (1) is located in the roof, with in the lesser wing of the sphenoid. The floor is separated from the lateral wall by the inferior orbital fissure. (b) Drawing illustrates the axial anatomy of the globe. On imaging, it is not possible to distinguish sclera, choroids, and retina, unless retinal or choroidal detachment is present. The lens separates the aqueous humor from vitreous humor
Orbit is a pyramid-shaped structure, constituted by seven bones. The medial wall is the thinnest and has four bones, namely, frontal process of maxilla, lacrimal bone, sphenoid, and lamina papyracea of the ethmoid. The lateral wall is constituted by the sphenoid wings and zygoma. The orbital roof is constituted by the orbital process of the frontal bone and lesser wing of the sphenoid. The floor is the weakest wall, constituted by maxilla, zygoma, and palatine bones.
Anterior chamber (AC) is crescent shaped between the lens and the cornea, measuring 2.5–3.5 mm in depth (Fig. 19.1). It is isointense to the vitreous on T1- and T2-weighted sequences. The posterior chamber lies between the posterior surface of the iris and anterior surface of the vitreous.
The vitreous constitutes 2/3rd volume of the eye (4 cc) and serves as the shock absorber. Because of 98 % water content, it has longer relaxation times than most tissues but shorter than that of water.
The intraocular lens measures 9 mm diameter and 4 mm in thickness. Anterior to the lens is the aqueous humor and posterior to the lens is the vitreous humor. It is the least hydrated organ (67 %) in the body and is therefore darker on MRI than surrounding tissues.
The walls of the globe include sclera (outer layer), uvea (middle layer), and retina (inner layer). It is not possible to distinguish between these three layers on CT or MRI in normal eye. Tenon’s capsule surrounds the eyeball from optic nerve to the ciliary muscle.
Imaging
Radiographic assessment of the orbits can detect two-thirds of the orbital fractures but has very limited sensitivity for soft tissue injuries. Ultrasound is contraindicated in patients where there is suspicion of globe rupture. MRI is not the primary modality in the evaluation of intraocular foreign body due to risk of damage by motion of a ferromagnetic foreign body and artifact produced by ferromagnetic foreign bodies. MRI is contraindicated if there is suspicion of metallic foreign body in the orbit.
CT is the modality of choice for traumatized eye and suspected ferromagnetic foreign body due to its wide availability in emergency departments, rapid scan time, no/minimal motion artifact, and high sensitivity in detection of foreign bodies [3].
Imaging Protocol
CT: Orbital protocol (0.625–1.25 mm slice thickness)
Noncontrast CT
Performed as part of the facial CT in axial plane
Sagittal and coronal reformations performed at 1 mm interval
Soft tissue and bone algorithm reconstructions
MRI: Orbital protocol (3 mm slice thickness)
1.
Axial and coronal T1 through orbits without fat sat
2.
Coronal FSE T2 through orbits with fat sat
3.
Post-gadolinium axial T1 with fat sat through orbits
4.
Coronal T1 chiasm through globes with fat sat
5.
Sagittal T1, axial FLAIR, axial T2, axial DWI through whole brain
6.
Optional T1 axial through whole brain
Anterior Segment Injury and Lens Dislocation
Trauma accounts for more than half of the lens subluxation-dislocation. It is caused by disruption of the zonular attachments, which hold the lens in place. The lens is most commonly dislocated posteriorly, often lying in dependent vitreous humor. Spontaneous atraumatic dislocation, which is often bilateral, is associated with Marfan syndrome, homocystinuria, sulfite oxidase deficiency, hyperlysinemia, ED syndrome, aniridia, and congenital glaucoma. Most patients with lens dislocation will have a pars plana vitrectomy/lensectomy with an intraocular lens implantation.
The patients with traumatic hyphema have hemorrhage in anterior chamber, usually from tear of ciliary body and iris. Posttraumatic cataract is most often localized and not associated with significant loss of vision [4].
Imaging: Anterior chamber injuries are characterized by decrease in the depth of the anterior chamber, when compared with the normal eye. A dislocated lens is seen as high attenuation lenticular structure in the vitreous on CT, where it is generally free floating (Figs. 19.2 and 19.3). A ruptured lens capsule often results in decreased attenuation and subtle increase in the size of the lens.
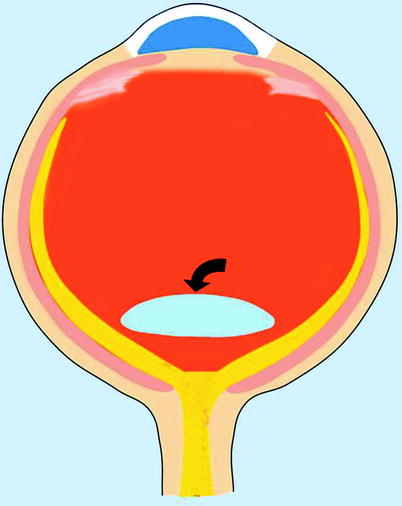
Fig. 19.2
Intraocular dislocation. Drawing illustrates the dislocated lens located posteriorly in the vitreous chamber
Fig. 19.3
Lens dislocation from penetrating trauma. (a) Axial CT shows posterior subluxation of the lens, increase in the depth of the anterior chamber, and vitreous hemorrhage (arrowhead). (b) Superior dislocation of the right lens (arrowhead) seen in a patient with right lateral orbital wall fracture and overlying soft tissue contusion from blunt trauma
Open-Globe Injury
Traumatic rupture of the globe results in loss of vitreous and posterior displacement of lens, causing deepening of the anterior chamber. Vitreal prolapse is associated with retinal detachment (RD), iridodialysis or ciliary body cleft, and contusion cataract (41 %) [5]. Globe ruptures (5 % of blunt injuries) are associated with grades III and IV hyphema.
Superior nasal limbus is the most common site of globe rupture because lower temporal quadrant is the most exposed site to trauma. The risk of trauma-induced globe ruptures is highest in eyes after cataract surgery and in females. The rupture of the globe most often occurs at the site of insertion of intraocular muscles because the sclera is thinnest at this site.
Imaging: The CT findings of globe rupture include vitreous hemorrhage, globe contour deformity, obvious loss of globe volume, absence of lens, intraocular air/foreign body, scleral discontinuity, increased depth of anterior chamber, and RD/CD (Figs. 19.4, 19.5, 19.6, 19.7, and 19.8). Flat tire sign is characterized by flattening of the posterior contour of the globe due to posterior collapse of the sclera and volume loss in the vitreous chamber.
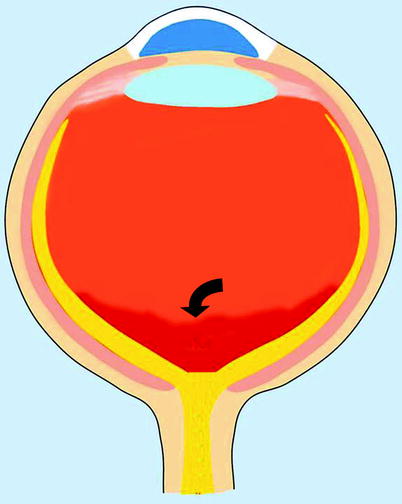
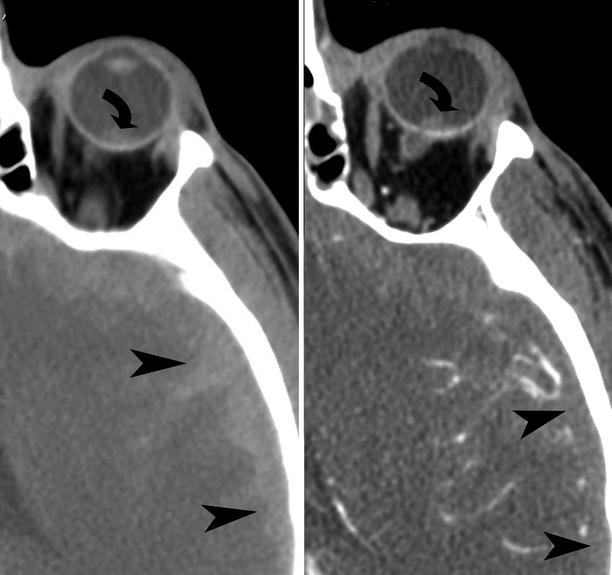
Fig. 19.4
Ruptured globe. Drawing illustrates the imaging findings of distorted outline of the globe, increase in the depth of the anterior chamber with posterior location of the lens, and vitreous hemorrhage
Fig. 19.5
Traumatic globe rupture. (a) Bilateral ruptured globes and orbital blowout fractures from wrench chain trauma. Axial CT shows bilateral open-globe injuries with vitreous hemorrhage. There is obvious distortion of the outline of the left globe (arrowhead). The right intraocular lens (arrow) is dislocated in to the vitreous chamber. There are bilateral blowout fractures involving the medial orbital walls (curved arrows). (b) Axial CT demonstrates globe rupture caused by shrapnel from a pipe bomb explosion. There is gross contour deformity and deflation of the globe (arrowhead). There is intracranial hemorrhage (curved arrow) caused by the shrapnel
Fig. 19.6
Right globe rupture from bullet injury. (a) Axial CT shows increase in the depth of the anterior chamber (curved arrow), extensive vitreous compartment hemorrhage, and distortion in the shape of the globe (straight arrow). (b) Axial CT of the cerebral hemisphere shows the track of the bullet illustrated by bone fragments (curved arrows)
Fig. 19.7
Vitreous chamber hemorrhage. Drawing illustrates vitreous chamber hemorrhage (curved arrow), which can be an isolated finding or associated with globe rupture, lens dislocation, or orbital fractures
Fig. 19.8




Vitreous chamber hemorrhage from blunt trauma in a 28-year-old male. Noncontrast axial CT and contrast-enhanced CT demonstrate left vitreous hemorrhage (curved arrows), left subdural hemorrhage (arrowheads)
Related posts:



Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
