Fig. 17.1
Normal CT anatomy and facial buttresses. (a) 3D surface-rendered image demonstrating the four vertical and four transverse buttresses (1 medial maxillary, 2 lateral maxillary, 3 upper transverse maxillary, 4 lower transverse maxillary, 5 posterior vertical, 6 upper transverse mandibular, 7 lower transverse mandibular, and 8 posterior maxillary). (b, c) Axial CT demonstrates the normal anatomy of the facial bones (arrowhead zygomatic arch, curved arrow laminae papyracea, white straight arrow optic canal, black straight arrow anterior clinoid process, star greater wing of sphenoid, and white arrow superior orbital fissure)
The floor of the anterior cranial fossa (ACF) is formed by the cribriform plate of the ethmoid, the frontal bone, and the lesser wing of the sphenoid. The frontal bone forms the majority of the floor of the ACF and also comprises the majority of the orbital roof. The lesser wing of the sphenoid forms the posterior margin of the ACF. The floor of the middle cranial fossa (MCF) is formed by the greater wing of the sphenoid and the squamosal portion of the temporal bone [7].
Orbital Fractures
The orbit is shaped like a cone with the apex posterior and the base anterior. The apex of the orbit is at the convergence of the superior and inferior orbital fissures. The anterior orbital rim is composed of the frontal, maxillary, and zygomatic bones.
Fractures of the orbit can affect the orbital rim, orbital walls, or orbital apex. Orbital apex fractures are an important fracture to detect due to proximity to the optic nerve and are more commonly seen with complex injury. The most common isolated orbital fractures are the so-called blowout fractures that occur in the medial and inferior orbital walls.
Blowout Fracture
A blowout fracture is a fracture of the orbital wall that displaces outwardly. In 1957 Smith and Regan proposed a mechanism of increased intraorbital pressure secondary to a direct frontal blow to the globe [8]. The forces are transmitted through the orbital walls with fracturing of the weakest sections while the orbital rim remains intact [9]. The lamina papyracea is the thinnest bone but is reinforced with buttressing from the ethmoid air cells. The inferior orbital wall is made weaker by the presence of the infraorbital groove and is the most common site of a fracture. The fracture fragment can displace inferiorly into the maxillary sinus, resulting in herniation of intraorbital fat, and/or extraocular muscles. The “trapdoor” blowout fracture, which is more common in pediatric age group, occurs when the hinge fragment springs back into place often trapping the inferior rectus muscle. Entrapment of the inferior rectus muscle results in limitation of upward/outward gaze, while entrapment of the medial rectus muscle results in limitation in the lateral gaze.
The coronal and sagittal reformations are most useful for detecting orbital floor fracture. Axial and coronal images best detect fractures of the medial wall (Figs. 17.2 and 17.3). It is important to note the site of fracture, fracture displacement and/or fracture angulation, and the presence or absence of herniated orbital contents.
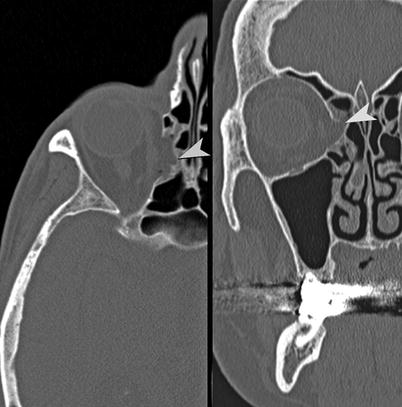
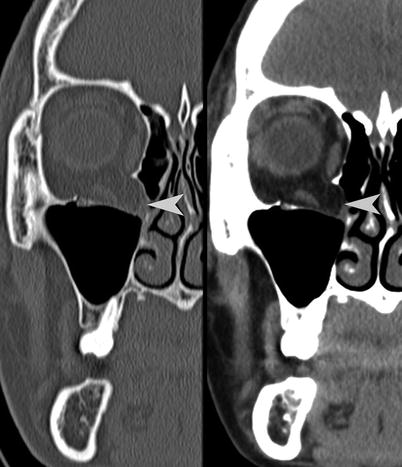
Fig. 17.2
Medial orbital wall blowout fracture. Axial and coronal CT images demonstrate a fracture (arrowhead) of the right medial orbital wall (lamina papyracea). Note the herniation of orbital fat through the defect in the right medial orbital wall
Fig. 17.3
Orbital floor lateral hinge blowout fracture. Coronal and sagittal images in bone and soft tissue algorithm demonstrating a right orbital floor blowout fracture. The displaced fragment hinges laterally at the infraorbital fissure. Note herniation of the orbital contents (arrowhead), including the inferior rectus muscle
Blow-in Fractures
The blow-in fracture is an inwardly displaced fracture of the orbital wall and/or rim resulting in a reduced orbital volume. These are generally the result of high-energy trauma and are most commonly seen in association with other fractures [10, 11]. A “pure” blow-in fracture is one limited to the orbital walls while the orbital rim remains intact (Figs. 17.4 and 17.5). “Impure” blow-in fractures, which are much more common, involve inward displacement of the orbital rim. Superior rim fractures, owing to their location and higher-impact forces, are usually more severe and associated with head injuries and frontal sinus fractures. Inferomedial blow-in rim fractures are the most common and seen with NOE fractures.
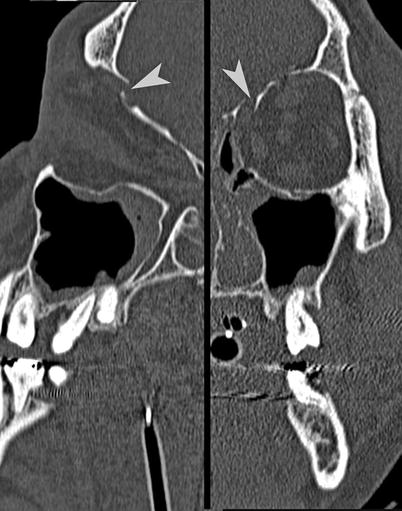
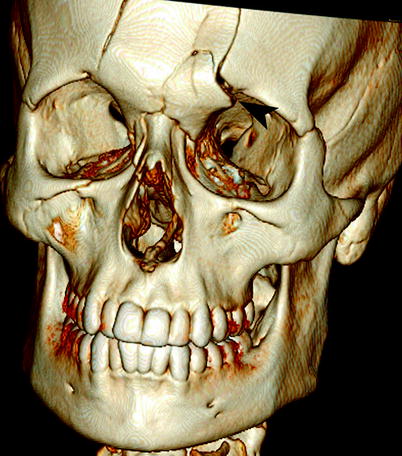
Fig. 17.4
Orbital roof blow-in fracture. Coronal and sagittal CT reformations demonstrate a “pure” orbital blow-in fracture (arrowhead) of the left orbital roof. The orbital rim is intact
Fig. 17.5
Orbital rim blow-in fractures. Surface-rendered image demonstrating orbital rim blow-in fracture of the superomedial orbital rim associated with a frontal fracture (arrowhead)
Fractures of the orbital apex may result in superior orbital fissure syndrome [12]. Symptoms include diplopia, ophthalmoplegia, ptosis, proptosis, and anesthesia in the ophthalmic nerve distribution. If there is associated blindness due to optic nerve injury (optic canal), it is termed orbital apex syndrome.
Zygoma Fractures
The zygoma (malar bone) is a dense solid bone that articulates with the frontal, maxillary, sphenoid, and temporal bones and forms the malar prominence (cheek), an important component of the facial contour. Since the zygoma is a solid bone, a direct blow to the cheek usually results in fractures of its relatively weaker articulation points. As the majority of the lateral orbital wall is formed by the zygoma, fractures to this region usually involve the orbit.
Zygomaticomaxillary Complex (ZMC) Fractures
While it is also called malar, tripod, tetrapod, and zygomatic complex fracture, the generally accepted and most commonly used term is zygomaticomaxillary complex (ZMC) fracture. It has a tendency to fracture at the weaker articulations with the frontal, sphenoid, maxillary, and temporal bones, resulting in disruption of the lateral maxillary and upper transverse maxillary buttresses [13].
While damage to the infraorbital nerve will result in loss of sensation to the eyelid and lateral nose, injury to the zygomatic nerve will result in sensory impairment to the lateral midface. Displaced fractures may result in flattening of the malar prominence and facial asymmetry.
Because of its complex articulation, the ZMC fragment can rotate in any plane along the fracture lines. The goal of imaging is to evaluate the extent of the fractures, the position and displacement of the ZMC fragment, and the status of the zygomatic arch (Figs. 17.6 and 17.7). The fractures may be associated with ocular injuries.
Fig. 17.6
ZMC fracture. (a, b) Axial and coronal CT demonstrates fractures of the anterior/posterolateral antral walls (arrowheads), orbital floor, lateral orbital rim, and zygomatic arch (curved arrow). (c) Surface-rendered image demonstrates fractures of the left zygomaticotemporal suture (curved arrow), zygomaticofrontal suture (straight arrow), and zygomaticomaxillary suture (arrowhead)
Fig. 17.7
Displaced and angulated ZMC fracture. (a, b) Axial image and surface-rendered image showing the zygoma complex posterolaterally displaced and internally rotated with displaced zygomaticomaxillary fracture (arrowheads) and zygomaticotemporal fracture (curved arrows). There is also fracture of the coronoid process of the mandible
Isolated Fractures
A focused direct blow may result in an isolated arch fracture. The direction of the force usually results in a depressed V-shaped fracture with the apex directed toward the infratemporal fossa. Segmented fractures may result as well (Fig. 17.8). Complications result from impingement of the temporal muscle and injury to the zygomatic nerve.
Fig. 17.8
Zygomatic arch fracture. (a, b) Axial CT and surface-rendered image demonstrates a depressed, segmental fracture of the zygomatic bone (curved arrows)
Nasal Fractures
The bridge of the nose is formed by the paired nasal bones, the frontal process of the maxilla, and the nasal processes of the frontal bone. The ethmoid is comprised of multiple delicate buttressing bones and air cells and is bounded laterally by the orbits and maxillary sinuses. The nasal septum is formed by the vertical plate of the ethmoid and vomer posteriorly and cartilaginous septum anteriorly. The lateral nasal wall is formed by three longitudinal elevations called conchae (turbinates). The superior and middle turbinates are part of the ethmoid, while the inferior turbinate is a separate bone.
The nasal bones form a portion of the nasal bridge and, if fractured, may result in facial deformity. Injury can range from isolated nasal bone fractures to more complex patterns involving multiple bones (Fig. 17.9). Radiographs are still routinely ordered if there is suspicion of an isolated nasal fracture. On CT attention to the nasal septum is important to evaluate for the presence of a septal hematoma, which may lead to complications of ischemic necrosis or abscess formation. Associated anterior nasal spine fractures may be present.