Fig. 25.1
Positioning of endotracheal tube when carina is obscured on a radiograph. Schematic representation of the left aortic arch outline which when extended horizontally at its inferior limit gives the landmark where the endotracheal tube should be placed. There is a nasogastric tube tip seen in the left bronchial tree
The radiographic findings of a right main stem bronchial intubation include hyperinflation of the right lung, atelectasis of the left lung, and atelectasis of the right upper lobe (with a right lower lobe intubation) (Fig. 25.2). Repositioning of the endotracheal tube in the trachea leads to rapid reexpansion of the collapsed lung in patients where inadvertent main stem bronchial incubation was performed.
Fig. 25.2
Bronchial intubation. (a) Portable chest radiograph demonstrates the tip of the endotracheal tube (arrowhead) extending into the right main bronchus. There is lack of aeration in the left hemithorax with collapse of the left lung. (b) Follow-up chest x-ray after repositioning of the endotracheal tube into the trachea demonstrates reexpansion of the left lung. A left-sided chest tube was surgically placed based on the clinician’s interpretation of the chest radiograph. (c) Intraoperative radiograph of the chest and abdomen, obtained during laparoscopic cholecystectomy, demonstrates right main bronchial intubation (arrow) with secondary collapse of the left lung
Other complications of endotracheal intubation include pneumothorax, tracheal rupture, tracheal stenosis (secondary to ischemia), and esophageal intubation (Fig. 25.3). The balloon cuff of the endotracheal tube should fill but not distend the lumen of the trachea. The ratio of balloon cuff diameter to tracheal diameter of more than 150 % is a predictor of tracheal damage [5].
Fig. 25.3
High placed endotracheal tube. (a) Sagittal CT reformation demonstrates the cuff (arrowhead) of the endotracheal tube inflated in the hypopharynx. The upper esophagus is outlined by air from the endotracheal tube. (b) Coronal CT reformation of the abdomen demonstrates gaseous distention of the stomach and small bowel loops due to air leaking from the endotracheal tube
The imaging findings of esophageal intubation include endotracheal tube cuff diameter more than that of the trachea, distention of the bowel lumen, and presence of air column in the esophagus. If an esophageal intubation is suspected, then a chest radiograph should be done after rotating the head to the right side and turning the patient to the right side by 25°. This obliquity results in esophageal air column projecting separate from the tracheal air column.
Tracheostomy Tube
Tracheostomy tube is used for long-term ventilation or in patients with laryngeal obstruction. Its caliber should be two-thirds the caliber of the trachea. It should be inserted at the level of the third tracheal cartilage with the tip placed above the level of the carina. It is not unusual to see pneumomediastinum and subcutaneous emphysema after placement of a tracheostomy tube. The complications include tracheal perforation, fistulous communication between trachea and esophagus, and malpositioning (Fig. 25.4).
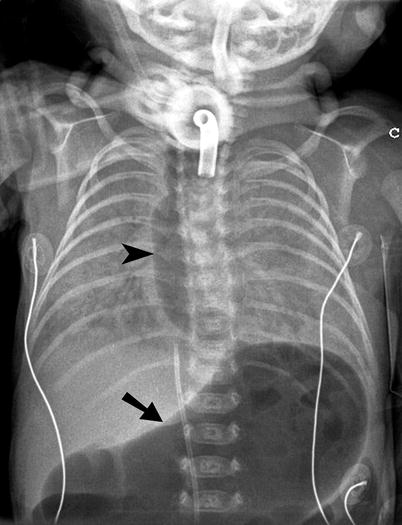
Fig. 25.4
Abnormal tracheostomy tube positioning. Plain radiograph of the chest and upper abdomen demonstrates marked distention of the esophagus (arrowheads) and stomach (arrow) due to leakage of air from the tracheostomy tube into the upper gastrointestinal tract
Nasogastric Feeding
Nasogastric tube is widely used to decompress the acidic gastric contents and reduce aspiration risk. It is recognized by the presence of a radiopaque line traversing the entire tube length. The side port of the nasogastric tube is approximately 8 cm from the tip. Ideal location of the nasogastric tube is in the stomach with the side port below the gastroesophageal junction. If the side holes of the tube are located in the distal esophagus, it can lead to aspiration pneumonia.
A feeding tube is recognized by the presence of a linear radiopaque tungsten band at the tip of the tube. It is ideally place in the distal duodenum and is used for enteric feeding without the risk of gastroesophageal reflux. Placement of the tip distal to the gastric pylorus reduces the risk of aspiration.
The enteric tubes may be coiled in the pharynx, esophagus, or stomach. The may be malpositioned into the bronchial tree, mediastinum, or pleural space (Fig. 25.5). If the post feeding tube or nasogastric tube placement radiograph shows placement in the tracheobronchial tree, the tube should be withdrawn and a follow-up radiograph obtained to rule out a pneumothorax [6]. Rare complications include esophageal perforation and swallowing of entire enteric tube.
Fig. 25.5
Abnormal nasogastric and feeding tube positions. (a) Plain radiograph demonstrates a feeding tube (arrow) extending through the right main bronchus and penetrating into the pleural space. (b) Plain radiograph demonstrating feeding tube extending coiled in the left main bronchus and the tip (arrowhead) extending into the right main bronchus. (c) Plain radiograph demonstrating nasogastric tube (arrowhead) extending into the right lower lobe bronchus. (d) Plain radiograph demonstrating coiling of the nasogastric tube (arrow) in the hypopharynx. (e) Plain radiograph of the abdomen demonstrating tip of the feeding tube in the stomach on the first study and in the distending colon (arrow) on the second study. The patient had swallowed the feeding tube between the two studies
G and GJ Tubes
G and J tubes are widely used for long-term enteric feeding, often used in patients with failure to thrive, risk of aspiration, swallowing dysfunction. There are an increasing number of these tubes placed by interventional radiologist because of the advantage of their placement without the need for general anesthesia. There is 5 % major complication rate associated with G-tube placement [7]. The complications include colonic perforation, tube dislodgement, tube migration, peritonitis, abscess formation, septicemia, tube site insertion infection, and GI bleeding (Fig. 25.6).
Fig. 25.6
G-tube malposition. (a) Tube injection study demonstrating the G tube located outside the stomach. There is contrast extravasation outside the bowel loops (arrowheads). There is free air (curved arrow) under the right dome of diaphragm. (b) Noncontrast CT after tube injection demonstrates the G tube (arrow) located in the left anterior abdominal wall. The contrast (arrowhead) injected through the G tube is present within the peritoneal cavity, anterior to the left lobe of the liver and the stomach. (c) Left gastric arteriogram demonstrates active arterial bleeding (arrow) after gastrojejunostomy tube insertion. (d) G-tube injection study demonstrates opacification of the colonic lumen from inadvertent colonic perforation
Central Venous Catheters
More than five million central venous catheters are placed by physicians in the USA, most often by surgeons and anesthesiologist, without image guidance [8]. While tunneled catheters are most often placed by surgeons or interventional radiologists, nontunelled catheters are most commonly placed by the surgeons and anesthesiologists. In 1999, interventional radiologists accounted for 20 % of the tunneled and 15 % of the nontunelled catheters placed in Medicare patients [9].
The subclavian vein is separated from the subclavian artery by anterior scalenus muscle. The subclavian vein is separated from the pleura of the lung apex by only 5 mm. The needle placement at the time of subclavian central venous catheter insertion should be in inward and slightly upward direction (from the mid clavicle, aiming toward the sternoclavicular joint).
Imaging plays an important role in documenting correct position of the central venous line tip as between 10 and 30 % of the catheters placed without imaging guidance are in suboptimal position. The right tracheobronchial angle is the best anatomic landmark to delineate the border of the superior vena cava and right atrium junction. The optimal position of central line tip is in the superior vena cava, adjacent to the cavoatrial junction. If the central venous line tip is placed too high from the cavoatrial junction, the tip may be above the venous valves or may be outside the vascular lumen. The valves are found in the subclavian vein and internal jugular vein, approximately 2.5 cm from their confluence to form the brachiocephalic vein. The placement of the catheter tip above the valves can lead to inaccurate measurement of central venous pressures (most commonly elevated pressures).
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


