Fig. 11.1
Schematic illustration of the anatomy of the thoracic cage. 1R first rib, 2R second rib, C clavicle, CC costal cartilage, CM costal margin, ICJ interchondral joint, M manubrium of the sternum, MSJ manubriosternal joint, SN suprasternal notch, XSJ xiphisternal joint
11.3.1.2 Sternoclavicular Joint
The sternoclavicular joint (SCJ) is a synovial sellar joint and represents the only skeletal articulation between the axial skeleton and the upper limbs (Johnson 2008). The joint is completely divided by an articular fibrocartilaginous disc and comprises the sternal end of the clavicle, cartilage of the first rib, and the clavicular notch of the manubrium, as well as the fibrous capsule, anterior and posterior sternoclavicular ligaments, interclavicular ligament, and the costoclavicular ligament (Johnson 2008). These ligaments provide stability to the joint (Fig. 11.2).
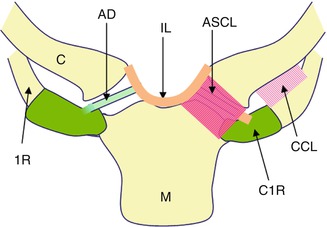
Fig. 11.2
Schematic illustration of the anatomy of the sternoclavicular joint. 1R right first rib, C1R cartilage of left first rib, C right clavicle, CCL costoclavicular ligament, AD articular disc, IL interclavicular ligament, ASCL anterior sternoclavicular ligament, M manubrium
11.3.1.3 Ribs and Associated Joints
The first to seventh ribs articulate to the sternum by costal cartilages (Fig. 11.1). The cartilages of the first to tenth ribs join the superjacent costal cartilage, whereas the 11th and 12th ribs have a free anterior end. Slight gliding movements occur at sternocostal joints to allow for ventilation. The sixth to ninth costal cartilages articulate via synovial joint with a fibrous capsule, and these interchondral joints are strengthened by interchondral ligaments (Gatzoulis 2008). Costal cartilages are connected to the ribs via the costochondral junction, at which no movement occurs. Posteriorly, the head of the first and tenth to 12th ribs articulates with the corresponding vertebral body by a simple synovial joint (costocorporeal joint). In the others, an intraarticular ligament bisects the joint, producing a double synovial compartment (Gatzoulis 2008). For the first to tenth ribs, the facet of a costal tubercle articulates reciprocally with the transverse process of its corresponding vertebra, forming the costotransverse joint. Strong ligaments binding the costocorporeal and costotransverse joints allow only slight gliding along the shape and direction of the articular surfaces at these joints (Gatzoulis 2008).
11.3.2 Injuries of the Thoracic Cage
11.3.2.1 Injuries of the Sternum, Manubriosternal Joint, and Xiphisternal Joint
Sternal fractures are rare thanks to the elastic recoil of the ribs which suspend the sternum (Gatzoulis 2008). A blow from the front may lead to sternal contusion (Fig. 11.3), fracture, and MSJ disruption/dislocation (Fig. 11.4). There are two mechanisms of MSJ dislocation (Fig. 11.5). Type I is a posterior dislocation of the sternal body as a result of direct impact to the body, e.g., direct compression injury following a scrummage or being tackled from the front while running forward (Fowler 1957). Type II is a posterior dislocation of the manubrium, which follows a flexion-compression injury of the thorax and neck, i.e., the neck is hyperflexed forward forcibly and the chin, clavicles, or the upper two ribs push the manubrium backward (Nikas et al. 1995). Isolated MSJ dislocation as a match injury in rugby players has been reported on a case basis (Smith et al. 2001). Sternal fractures may be associated with rib fractures and, in severe cases, with internal injuries such as pneumothorax and pulmonary and cardiac contusion (Celik et al. 2009).
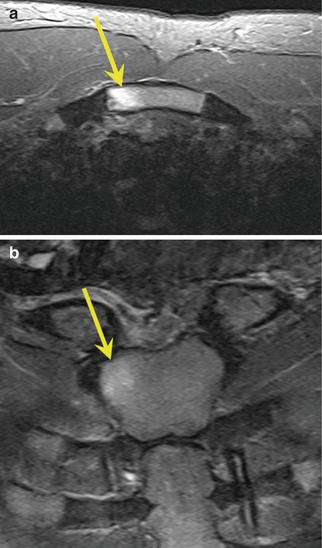
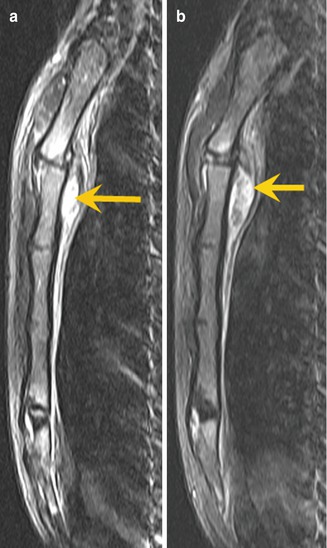
Fig. 11.3
Example of a contusion injury. A 20-year-old male rugby player who complained of upper chest pain immediately after a scrummage during a rugby match. Radiography did not show any obvious fracture of the thoracic cage (not shown). However, (a) axial and (b) coronal STIR MRI show abnormal hyperintensity in the right superior corner of the manubrium (yellow arrows), indicating a bone contusion of the manubrium
Fig. 11.4
Example of manubriosternal disruption. A 21-year-old male rugby player was tackled from the front during a rugby match. (a) Sagittal STIR and (b) T1-weighted MRI show a fluid collection directly adjacent to the posterior cortex of the manubrium, immediately below the manubriosternal joint (yellow arrows). It shows hyperintensity on both STIR and T1-weighted images, consistent with recent hematoma
Fig. 11.5
Two types of manubriosternal joint dislocation. (a) Type I is a posterior dislocation of the sternal body as a result of direct impact to the body, e.g., direct compression injury following a scrummage or being tackled from the front while running forward. (b) Type II is a posterior dislocation of the manubrium, which follows a flexion-compression injury of the thorax and neck, i.e., the neck is hyperflexed forward forcibly and the chin, clavicles, or the upper two ribs push the manubrium backward
Imaging diagnosis of sternal injury can be made by plain films, computed tomography (CT), and MRI. A lateral radiograph may demonstrate MSJ dislocation (Smith et al. 2001). CT can detect subtle fracture lines which may not be clearly seen on plain films. MRI allows detection of associated soft tissue injuries as well as the presence of any bony contusion injury and hematoma around the injury site (Figs. 11.3 and 11.4). For MRI, a patient should be placed in a prone position if possible, with the use of a cardiac/large surface coil. Imaging sequences should include short tau inversion recovery (STIR), or similar fluid-sensitive fat-suppressed fast spin echo sequences, and T1-weighted sequences in axial, sagittal, and oblique coronal planes.
11.3.2.2 Injuries of the Sternoclavicular Joint
The transmission of forces along the clavicle tends to cause clavicular shaft fracture rather than SCJ dislocation (Chaudhry et al. 2011), making SCJ dislocation a rare entity, accounting for only 3 % of shoulder girdle injuries (Gilot et al. 2006). Posterior dislocations are less common than anterior dislocations with a reported incidence ranging between 5 and 27 % of all SCJ dislocations (Gilot et al. 2006). SCJ posterior dislocations occur during a fall on the lateral aspect of the shoulder (Thomas et al. 1999; Marcus and Tan 2011; Mirza et al. 2005) (Fig. 11.6).
Fig. 11.6
Sternoclavicular joint posterior dislocations occur during a fall on the lateral aspect of the shoulder
Injury of the SCJ may not be obvious on plain films, but CT or MRI is usually diagnostic (Chaudhry et al. 2011) (Figs. 11.7, 11.8, and 11.9). The role of ultrasound for diagnosis of SCJ injuries is equivocal as the reported sensitivity is low and confirmation of the diagnosis by CT is commonly required (Blakeley et al. 2011; Pollock et al. 1996). Posterior dislocation of the clavicle can cause potentially hazardous injuries due to proximity to mediastinal vascular structures, the trachea, and esophagus. Clinical assessment of patients with SCJ injury should include the presence of dyspnea, dysphagia, hoarseness (Chaudhry et al. 2011), upper extremity weakness due to brachial plexus injuries, and myocardial conduction abnormalities (Wirth and Rockwood 1996). Complete obstruction of the brachiocephalic vein and impingement of the aorta (Mirza et al. 2005) and cerebrovascular accident (Marcus and Tan 2011) as a result of rugby injuries have been reported. When necessary, contrast-enhanced imaging will help to clarify the anatomical relation of the dislocated clavicle and the brachiocephalic arteries and veins, as well as the aorta (Chaudhry et al. 2011).
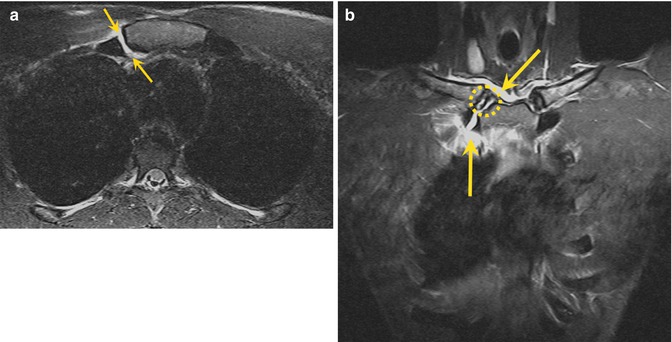
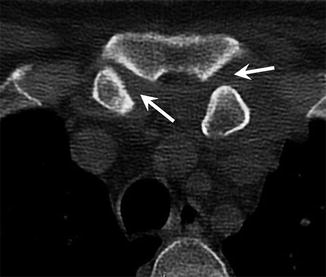
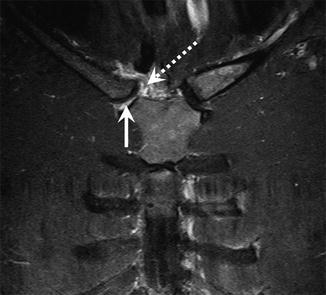
Fig. 11.7
A 22-year-old male rugby player with capsular joint injury suggesting right sternoclavicular joint dislocation. Correct articulation at the time of imaging. (a) Axial and (b) coronal STIR MRI show the disrupted right sternoclavicular joint capsule (yellow dotted circle) with hyperintense fluid-equivalent signal extending from the joint into the surrounding soft tissues (yellow arrows). No bony injury is seen
Fig. 11.8
A 49-year-old male rugby player with bilateral persistent posterior sternoclavicular joint dislocation at the time of imaging. Axial high-resolution CT image shows posterior dislocation especially on the left and discongruity of the joint on both sides with a widened joint space (arrows)
Fig. 11.9
A 21-year-old male rugby player after right sternoclavicular joint dislocation. Coronal STIR MRI shows joint capsule disruption with periarticular high-intensity hematoma (dotted arrow) and fluid within the joint space (arrow)
11.3.2.3 Injuries of the Ribs and Associated Joints
Traumatic stress is often the result of compression of the thorax, and thus the usual site of fracture is at the weakest point of the rib, i.e., just in front of the angle (Gatzoulis 2008). Costochondral injuries are commonly seen in the middle to lower ribs following a direct anterolateral blow during a match (Fig. 11.10) (Lopez et al. 2013). An isolated first rib fracture (Vikramaditya 2001) and an injury to the first sternocostal joint can occur as a result of a direct blow to the posterolateral aspect of the shoulder in a powerful direct collision with an opponent’s shoulder during a tackle (Kemp and Targett 1999). These injuries may be missed or misdiagnosed as “anomalous articulation” on plain films (Vikramaditya 2001), and thus CT and MRI play an important role in the diagnosis of these lesions (Lopez et al. 2013; Kemp and Targett 1999). However, subtle chondral fractures may not be obvious even on CT (Fig. 11.11). Multiplanar reconstruction should be deployed in the acute stage to identify the injury and to visualize the anatomic relation of any associated injuries to the surrounding tissues (Willis-Owen, et al. 2009). Volume-rendered images (Fig. 11.10) are helpful for grasping the anatomical information in a three-dimensional fashion.
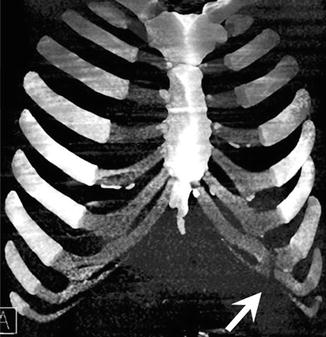
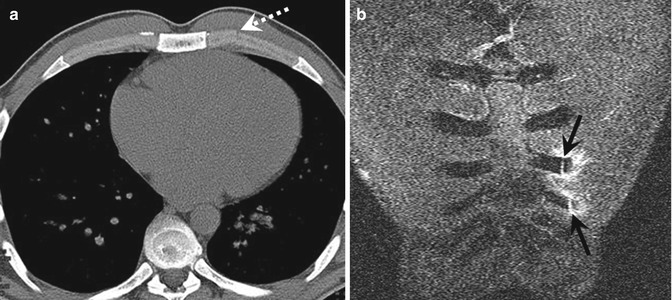
Fig. 11.10
Volume-rendered CT image of a 22-year-old male rugby player clearly demonstrates left seventh and eighth chondral fractures, with associated fracture of the interchondral joint between these two ribs (arrow)
Fig. 11.11
A 28-year-old male rugby player with subtle left fourth and fifth chondral fractures. (a) Fracture line (dotted arrow) can be seen on axial CT, but it is not obvious and can easily be missed. (b) Coronal STIR MRI, on the other hand, clearly depicts the fractures (black arrows) with associated fluid accumulation around the fracture sites
For MRI, patients should be in a prone position and a marker should be placed at the point of tenderness (Fig. 11.12). Axial and oblique coronal STIR images are particularly useful (Figs. 11.13 and 11.14). Because of breathing motion and cardiac pulsation, the presence of artifacts in the images is inevitable (Figs. 11.13 and 11.14). To minimize chest wall movement, patients should be advised to breathe gently with the use of diaphragmatic excursions (Hopper et al. 2010).
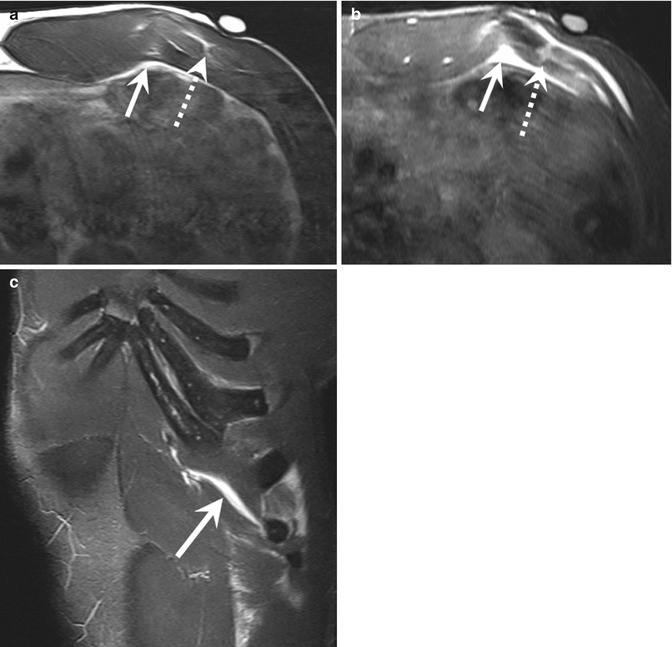
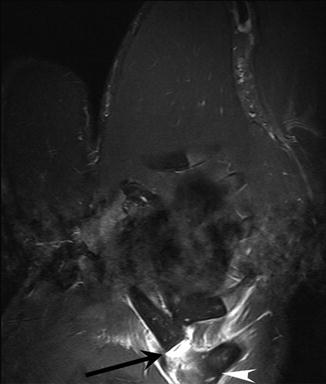
Fig. 11.12
A capsule containing oil is placed as a marker at the point of tenderness (arrow)
Fig. 11.13
A 26-year-old male rugby player with a left eighth chondral fracture with hematoma. Fracture line (dotted arrows) can be seen on both (a) axial T1-weighted and (b) STIR MRI. (b) Axial and (c) oblique coronal STIR MRI clearly depict the associated fluid accumulation around the fracture site, and T1-weighted image shows hyperintensity, consistent with hematoma (arrows)
Fig. 11.14
A 27-year-old male rugby player with a fracture of the left seventh costal cartilage (arrow). Oblique coronal STIR MRI demonstrates the site of fracture and surrounding hematoma. Inferior dislocation of lateral portion of chondral rib (arrowhead) is also seen
11.3.3 Anatomy of the Thoracic/Abdominal Muscles
Muscles around the thorax cover body parts from the neck to the upper abdomen. Intrinsic chest wall muscles include the intercostal muscles, subcostal, transversus thoracis, levatores costarum, and serratus posterior, all of which play a role in rib cage movement including ventilation (Gatzoulis 2008). A bony injury of the chest wall can damage these small muscles if the injury occurs at their attachment sites. Other muscles with direct attachments to the ribs or the sternum include the pectoralis major (Fig. 11.15), pectoralis minor, rectus abdominis (Fig. 11.16), serratus anterior, latissimus dorsi, transversus abdominis (Fig. 11.17), external/internal oblique (Fig. 11.17), levator costae, quadratus lumborum, erector spinae, scalenus, and subclavius muscles (Gatzoulis 2008).
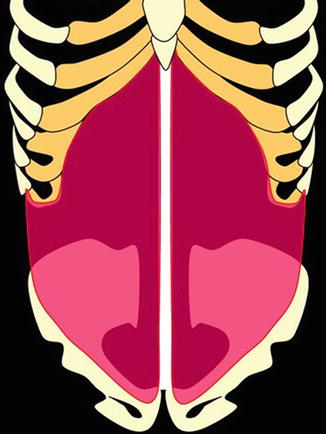
Fig. 11.15
Schematic illustration of the pectoralis major muscle showing its attachment to the thoracic cage. The clavicular head is attached to the anterior surface of the medial half of clavicle. The sternocostal head is attached to the anterior surface of sternum, first to sixth costal cartilages, and the aponeurosis of external oblique muscle
Fig. 11.16
Schematic illustration of the rectus abdominis muscle showing its attachment to the thoracic cage. It attaches to cartilages of the fifth to seventh ribs and the xiphoid process
Fig. 11.17
Schematic illustration of the transversus abdominis and oblique muscles showing their attachment to the thoracic cage. The transversus abdominis attaches to the inner surfaces of 7th–12th costal cartilages. The internal oblique muscle attaches to 10–12th ribs
11.3.4 Injuries of the Thoracic/Abdominal Muscles
Muscle injuries can be assessed by ultrasound or MRI (Figs. 11.18, 11.19, and 11.20). Ultrasound can be performed quickly in the emergency room or an outpatient clinic, facilitating a quick and dynamic imaging diagnosis. However, the examiner has to be aware that subtle grade 1 lesions may have a normal sonographic appearance in the acute stage (Koh and McNally 2007). MRI, on the other hand, has higher sensitivity to low-grade lesions, will give more detailed anatomical information, and enables imaging evaluation of deeper and a wider range of anatomical structures. For complete or partial tears of the pectoralis major, MRI has been shown to have excellent agreement with surgical findings (Carrino et al. 2000). It is important to recognize the severity of the muscle injury (complete or partial tear), as well as the location within the particular muscle because the therapeutic strategy will depend on the nature and location of the injury.
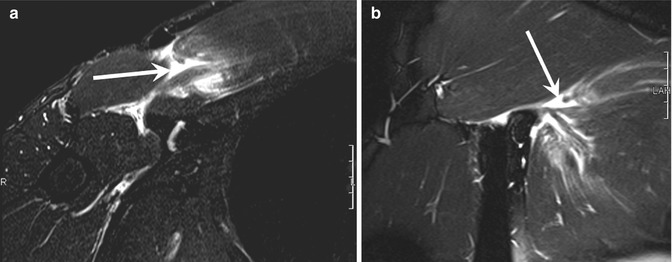
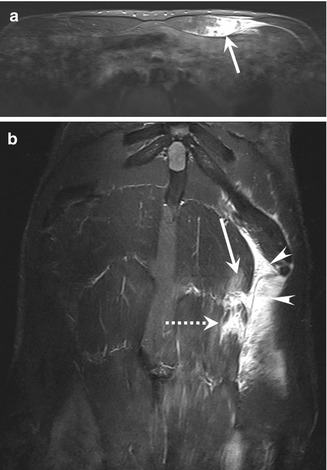
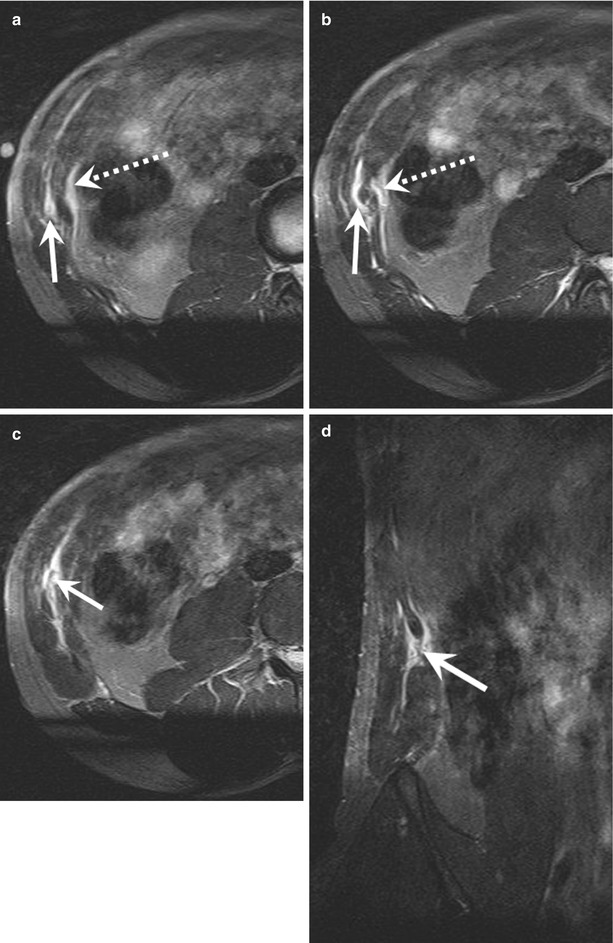
Fig. 11.18
A 40-year-old male rugby player with a right-side pectoralis major tear. (a) Axial and (b) coronal STIR MRI show intramuscular grade 2 strain with fiber disruption and hematoma (arrows)
Fig. 11.19
A 22-year-old male rugby player with left-side rectus abdominis tear. (a) Axial and (b) coronal STIR MRI show grade 2 lesion of the middle portion of left sided rectus abdominis (arrows) and grade 1 strain of the superior part (dotted arrow). Note marked intra- and extrafascial hematoma (arrowheads)
Fig. 11.20
A 25-year-old male rugby player with a right-side internal oblique muscle tear (grade 2). (a–c) Axial and (d) coronal STIR MRI show fluid-equivalent signal within right internal oblique muscle (arrows) and epifascial edema (dotted arrows)
Pectoralis major injuries are relatively rare injuries that occur primarily while lifting weights (Petilon et al. 2005), but can occur in a rugby match when a player receives a direct blow to the muscle during a tackle (Fig. 11.18). Pectoralis major injuries are known to occur following an eccentric contraction of the muscle as it is actively stretched (Connell et al. 1999) and during a fall with the arm abducted and extended (Rehman and Robinson 2005). A snap may be heard at the time of injury, followed by acute pain. A tear may be at the sternal and/or clavicular heads, intramuscular (Fig. 11.18), or at the musculotendinous junction, or the injury may be distal tendon avulsion (Petilon et al. 2005). Complete tears are most commonly avulsion injuries at or near the humeral insertion (Petilon et al. 2005), which require surgical repair, while partial tears can be treated conservatively (Connell et al. 1999). On plain films, soft tissue swelling can be seen and the pectoralis major shadow is absent; a bone fragment may be present at the humerus in case of humeral avulsion at the pectoralis insertion (Hopper et al. 2010). To achieve accurate localization of injury by ultrasound and MRI, imaging should be performed in the abduction and external rotation position to extend and improve visualization of the musculotendinous junction (Koh and McNally 2007). Ultrasound imaging longitudinal to the pectoralis muscle fibers shows fiber disruption, retraction, and possible hypoechoic or anechoic hematoma, most commonly involving the musculotendinous junction of the sternal head (Weaver et al. 2005). With MRI, a combination of sequences should be used for anatomical delineation (T1-weighted spin echo or proton density-weighted spin echo) and fluid detection (T2-weighted spin echo, T2-weighted fast spin echo with fat suppression, or STIR). Because of the robustness of STIR for homogeneous fat suppression, STIR is the sequence of choice in thoracic assessment of muscle edema (Carrino et al. 2000). Oblique coronal sequences along the long axis of the pectoralis major tendon are most useful for grading a tear (Connell et al. 1999). In chronic injuries, axial T1-weighted sequences are helpful for demonstrating scarring and atrophy (Ohashi et al. 1996).
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


