Fig. 15.1
Phantom foot mechanism involves the skier off balance, falling backward, unweighting the uphill ski and loading the inside edge tail of the downhill ski which results in sudden internal rotation torque on the knee loaded in flexion
Slip catch (valgus/internal rotation): This mechanism occurs when the skiers lose pressure on the outer ski during a turn. When the skier extends the outer lower limb to regain traction, the inside edge of the outer ski catches snow and decelerates abruptly forcing the knee into flexion and valgus and internal rotation under a compressive load. The skier falls backward and/or inward (Fig. 15.2) (Bere et al. 2013).

Fig. 15.2
Slip catch mechanism occurs during a turn, typically at high speed. The outer ski loses contact with the snow and drifts away from the skier, who extends the lower limb in an attempt to regain traction. The front inner edge of the ski catches the snow and forces the knee into flexion, internal rotation, and valgus under load as shown
Forward twisting (valgus–external rotation): This mechanism occurs when the skier’s center of gravity is forced forward (such as when the inner edge of a ski catches the snow and decelerates). It results in external rotation of the tibia, and with momentum, increasing flexion and valgus force is applied to the knee and can be magnified based on ski length and resultant torque (Fig. 15.3) (Järvinen et al. 1994). This is reportedly the most common mechanism of MCL sprain and ACL sprain in recreational skiers (Ganong 1996).
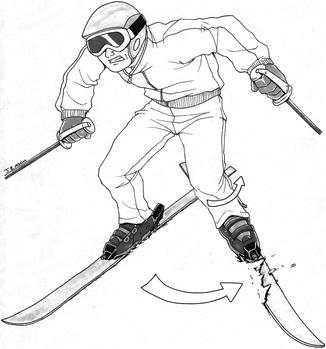
Fig. 15.3
Valgus-external rotation mechanism occurs when the skier’s center of gravity is forced forward, resulting in external rotation of the tibia, and with momentum, increasing flexion and valgus force on the knee
Boot–induced anterior drawer: Boot-induced anterior drawer is common in competitive freestyle and downhill skiers (Johnson 1988). ACL injury occurs when the tail of the ski contacts the snow first, with the ground reaction forces driving the ski tips and boot anteriorly creating a severe passive anterior drawer load on the tibia with respect to the femur (which is counter loaded by the posterior position of the skier and aggressive quadriceps loading (DeMorat et al. 2004)) (Rossi et al. 2003). A similar mechanism occurs when a stationary skier is struck from behind (Fig. 15.4) (Langran 2013).

Fig. 15.4
Boot-induced anterior drawer mechanism typically occurs after landing a jump, with initial contact of the tail of the ski with the snow and relatively extended knee. Ground reaction forces drive the ski tips and boot anteriorly and distally, creating a severe passive anterior translational force on the proximal tibia which is augmented by aggressive quadriceps contraction. The femur is counter loaded with posteriorly directed force produced by the relatively rear positioning of the skier and downward momentum from landing (see inset)
Ski lift–related knee injuries: Injury has also been described as skiers disembark a chair lift. It occurs when the tail of one ski is planted onto the ski of the person riding beside them. As they stand the weight of the ski causes the sharp edge to engage the soft plastic of the ski beneath. The forward and usually downhill momentum of the lift essentially results in a phantom foot-type scenario (Stoneham 2001).
Other mechanisms: Hyperextension injuries and traditional closed chain external rotation valgus mechanisms are encountered infrequently.
Imaging the Knee
Careful examination of all at-risk and clinically important structures in all 3 planes is necessary for accurate identification of injury (Boutin and Fritz 2005).
Given that a large proportion of MCL injuries are treated nonoperatively, the lack of surgical correlation of MRI findings means the sensitivity and specificity of MRI in their diagnosis are not well established. Axial and coronal planes provide the best visualization for assessment. Accurate description of the extent of injury to the superficial and deep components is potentially useful in determining the prognosis; entire superficial or combined superficial and deep injuries can be an indication for surgical management (Nakamura et al. 2003; Wilson et al. 2004).
The sensitivity and specificity of ACL disruption have both been variably recorded up to 100 % (Yoon et al. 2007; Behairy et al. 2009). More recently accuracy of approximately 95 % has been recorded with multiligamentous injuries and partial, chronic, or proximal injuries to the ACL accounting for erroneous interpretation (Rubin et al. 1998). Careful review of the fiber orientation, caliber, and continuity as well as abnormal signal intensity can help identify a partial tear. Particular attention should be paid to the proximal attachment of the posterolateral bundle and the proximal insertion generally, given its frequent involvement in ski-related ACL rupture (Ho et al. 1999).
MRI assessment provides approximately 93–96 % sensitivity and 88–90 % specificity for medial meniscal tears and 77–99 % sensitivity and 82–98 % specificity for the lateral meniscus, with no statistically significant difference in accuracy between 1.5 and 3.0 tesla platforms (Van Dyck et al. 2013).
15.2.2.2 Hip Injuries
Femoroacetabular impingement (FAI) is increasingly recognized as a cause of hip pain in the athletic population. Ganz et al. (2003) described 2 mechanisms by which soft tissue impingement at the hip joint occurs: cam-type deformity with bony overgrowth at the femoral head-neck junction which results in an aspherical femoral head and pincer-type deformity with overgrowth of the acetabular rim. In practice, concomitant features of both types are usually found. Whether a large proportion of the asymptomatic population have anatomic features of FAI is a matter of controversy, and the management paradigm is inconsistent among surgeons (Robinson 2012).
Hip dislocation is a rare but important injury requiring early orthopedic assessment. Anterior dislocations are more common among skiers (Matsumoto et al. 2003). In dislocations not associated with fractures, osteonecrosis of the femoral head is a serious complication (Flanigan et al. 2011).
Mechanism of Injury
While the hip is an inherently stable joint, the stresses sustained by the ligaments, labrum, and chondral surfaces of the hip as well as intrinsic anatomic features can predispose a skier to injury.
Herzog et al. reported a small case series of 36 painful hips in 29 professional alpine athletes, all of whom were found to have acetabular labral pathology and FAI, with approximately one third demonstrating chondral injuries at arthroscopy (Herzog et al. 2012). The group consisted of alpine skiers, Nordic (endurance) skiers, snowboarders, and aerial jumping athletes. All Nordic skiers reported an insidious onset of hip pain without traumatic incident, while racing and aerial athletes most commonly (40 %) reported a high-speed crash as the antecedent event. The second most common mechanism was gradual onset; lateral impact accounted for 8 % and dislocation reported in 8 % (Ho et al. 1999). Hip dislocations tend to occur secondary to a collision (Anderson et al. 2001).
Imaging of the Hip
While standard 3-plane proton density and fluid-sensitive sequences with and without gadolinium arthrography continue to be used, many centers are rethinking the use of invasive arthrography. The use of 3 tesla imaging of the hip in 3 planes with additional radial sequences can improve accuracy when identifying labral and “cam” pathology (Yoon et al. 2007). Regardless of method, focal chondrosis, labral tears or detachments, and the presence of cam or pincer deformities should be described and an assessment of acetabular anteversion should be performed.
Osteochondral fracture and bone contusion patterns that may indicate subluxation or dislocation as well as signs of potential complication, e.g., the double line sign of osteonecrosis, should be identified.
15.2.3 Upper Limb Injuries
The upper limb is injured in approximately 20 % of ski-related traumas (Davidson and Laliotis 1996; Westin et al. 2012). Thumb ulnar collateral ligament (UCL) sprains (“skier’s thumb”) account for approximately 10 % of all ski-related injuries and almost 40 % of upper limb traumas (Carr et al. 1981). Traumas to the shoulder girdle comprise 30 % of upper limb injuries including shoulder dislocation, clavicle and scapula fractures, soft tissue injury (including acromioclavicular [AC] joint separation and rotator cuff strain), and direct contusion. Shoulder dislocations are typically anterior and more commonly primary dislocators versus recurrent dislocators by a factor of 3–1 (Kocher et al. 1998). Apart from clavicle fractures which are increasing in frequency (Ganz et al. 2003), the incidence of shoulder injuries has remained relatively constant.
15.2.3.1 Thumb Injury
Mechanism of Injury
Skier’s thumb: The thumb ulnar collateral ligament is injured when the skier fails to release the ski pole during a fall. Maintaining the grasp results in forced extension and valgus loading of the thumb metacarpophalangeal joint (Hunter 1999). Note that the term “gamekeeper’s thumb” should be reserved for chronic laxity of the UCL through repetitive stress, not for acute injuries (Ritting et al. 2010). The contribution of the ski pole to the torque through the thumb probably contributes to more severe injuries; the ulnar expansion of the adductor aponeurosis becomes interposed between the displaced distal UCL and its attachment site (known as a Stener lesion). In fact, Stener lesions are more common in skiers than in the general population (Zeman et al. 1998).
Imaging of the Hand
Plain radiographic assessment of the thumb should be performed initially to identify any concurrent fracture (Tang 2011). In the presence of clinical instability and absence of fracture (controversy surrounds dynamic assessment in the presence of small avulsion fractures), radiography performed with valgus stress on the proximal phalanx can be used to evaluate instability (Louis et al. 1986). Radial deviation of more than 30–35° under stress is suggestive of UCL rupture (Heyman et al. 1993).
Stable (partial) UCL tears are usually man-aged conservatively, and thus, further imaging is usually not warranted. However, in the presence of instability requiring surgery, ultrasound or MRI can be performed.
Tears of the linear hypointense UCL band are diagnosed when high signal traverses a portion (partial tear) or the entire thickness (rupture) of the ligament (Boutin and Fritz 2005). Oblique-coronal plane sequences can be used to improve the visualization of the UCL (Boutin and Fritz 2005; Clavero et al. 2002). A Stener lesion has a characteristic “yo-yo” or “ball on a string” appearance with proximal and superficial (to the adductor aponeurosis) displacement of the UCL. MRI and ultrasound have both been reported to have sensitivity and specificity of up to 100 % (Melville et al. 2013; Hergan et al. 1995). While ultrasound is operator dependent, its proponents point out its ability to provide dynamic assessment as well as its efficiency and mobility (Fig. 15.5) (Melville et al. 2013).
Fig. 15.5
A 31-year-old male skier with a Stener lesions following a fall. (a) Transverse and (b) longitudinal ultrasound images of the thumb demonstrate displaced avulsion fragment (arrow) of the distal ulnar collateral ligament. The fracture fragment is displaced proximally and superficial to the adductor aponeurosis (open arrowheads) consistent with a Stener lesion. The proximal ligament is redundant and balled up adjacent to the metacarpal (closed arrowhead)
15.2.3.2 Shoulder Injuries
Mechanism of Injury
Shoulder dislocation: Axial loading via a fall onto an outstretched hand and abduction/external rotation torque applied to the shoulder by a ski pole caught behind the skier are typical mechanisms. The latter may be exacerbated by eccentric muscle contraction resisting the associated forced abduction (Herzog et al. 2012). Other potential causes include direct blows, collisions with other skiers or other stationary objects, or pole planting (Herzog et al. 2012). The ski pole (particularly with the wrist engaged in the strap) acts as an extension of the arm and increases the leverage and associated torque through the glenohumeral joint (McCall and Safran 2009).
Other injuries: Falls and direct blows to the anterior shoulder are the most common causes of clavicular, glenoid, and humeral fractures (more commonly proximal in skiers) (Bissell et al. 2008). AC joint injuries occur with falls in which the load is concentrated onto the acromion.
Imaging of the Shoulder
Plain radiographic assessment is the mainstay of initial imaging of the shoulder. Dislocation/subluxation of the glenohumeral and acromioclavicular joints; humeral, scapular, and clavicular fractures; and secondary signs of trauma (e.g., Hill-Sachs, osseous Bankart, and avulsive injuries) can be identified.
Assessment of glenohumeral joint instability post-dislocation can reveal a multitude of findings. MRI arthrography is considered more sensitive in the assessment of superior labrum anterior posterior (SLAP) and glenoid labral pathology (Magee 2009). Osteochondral injuries, joint effusion, bone contusion patterns related to dislocation, as well as associated impaction/avulsion fractures should be measured and described. Rotator cuff tears occur in 35 % of glenohumeral dislocations and in up to 100 % of dislocations that result in axillary neuropathy (Pevny et al. 1998).
15.2.4 Head and Spinal Injuries
Head injuries account for between 7 and 18 % (Ganz et al. 2003; Sulheim et al. 2011) of alpine skiing injuries. They account for the major cause of mortality (88 %) in snow sports and occur most frequently in younger, male skiers (Levy et al. 2002). Injuries range from concussion to severe intracranial hemorrhage and diffuse axonal injury.
The use of helmets has been shown to provide modest protective effects. There have been some concerns about an associated increase in neck injuries, but they were not borne out in subsequent studies (Anderson et al. 2001; Hagel et al. 1999, 2005; Sulheim et al. 2006; McCrory 2002). The International Ski Federation (Fédération Internationale De 2006) and many alpine sport districts strongly recommend wearing protective helmets, but few make it compulsory, other than for children in school skiing and snowboarding events and occasionally for lessons (Slaney et al. 2007). Nova Scotia in Canada mandates that all children and adults must wear helmets on the slopes. Standards for skiing and snowboarding helmets are controversial. New Canadian standards have been released that require helmets to be capable of sustaining multiple impacts. This is important as helmet damage is hidden beneath the outer plastic shell; it is difficult to assess the integrity of single-impact helmets that have been used previously. Currently very few helmets meet this standard (Sibbald 2012), and the utility of enforcing the use of potentially compromised helmets seems questionable.
Facial injuries: Injuries to the face account for up to 3 % of all ski-related injuries (Coury et al. 2013). Gassner et al. reported that of patients presenting with facial trauma, 42 % sustained injuries to their teeth and 23 % had facial bone fractures, many with concomitant soft tissue injury (Gassner et al. 2000). Tuli et al. reported 55 % of patients presenting with maxillofacial injuries had sustained facial fractures (77 % midface, 23 % lower jaw), an incidence similar to snowboarders, although skiers appeared more likely to sustain dentoalveolar trauma (Tuli et al. 2010). Men and those between 20 and 40 years were most susceptible to injury (Fédération Internationale De 2006; Slaney et al. 2007).
Spinal injuries: Spinal injuries represent approximately 3 % of all alpine skiing injuries (Levy and Smith 2000). Recent reports point toward an increasing trend for skiers to sustain more severe injuries and have a higher likelihood of neurologic sequelae (Franz et al. 2008). Skiers are reported to have a higher incidence of burst fractures followed by anterior compression fractures (Tarazi et al. 1999).
15.2.4.1 Mechanism of Injury
Falls (especially from ledges, jumps, and at the terrain park), collisions with other skiers/stationary objects, and lift accidents account for the vast majority of head and facial injuries (Slaney et al. 2007).
Earlier reports describe falls as the most common cause of spinal injury in skiers, although higher speed, higher likelihood of collisions, risk-taking behaviors and snowboarding style aerial maneuvers are postulated to account for increasing jump and terrain park-related spinal injuries in skiers (Coury et al. 2013). Forward falling mechanisms result in the trend toward more ski-related cervical spine injuries (Nakaguchi et al. 1999).
Lower back pain in alpine skiers and other athletes that correlates with vertebral body endplate lesions on imaging has been attributed to chronic biomechanical overload associated with jumping and high intensity training (Rachbauer et al. 2001).
15.2.4.2 Imaging of the Head and Spine
Given that the majority of head injuries sustained on the slopes are concussions, imaging findings will be limited. Initial imaging using CT scanning of the brain will be based on clinical grounds, but should determine the presence of intracranial hemorrhage or skull/facial fractures using standard trauma imaging protocols.
Routine CT and MRI trauma sequences of the spine should be obtained to assess disc, ligamentous, osseous, and spinal cord injury. Background risk factors such as degenerative and congenital spinal stenosis are more common in the cervical spine (Järvinen et al. 1994).
Chronic endplate lesions and “atypical Scheuermann disease” occur at the anterior or posterior margin of the vertebra as round, lucent defects with an irregular, sometimes fragmented sclerotic margin (Fig. 15.6). They most likely represent longstanding repetitive injury to the vertebral ring apophysis and occur most frequently at the thoracolumbar junction (Levy and Smith 2000). Only anterior endplate lesions appear to result in clinically significant back pain (Ogon et al. 2001).

Fig. 15.6
A young elite skier with anterior endplate lesions. Lateral lumbar spine radiograph demonstrates anterior endplate lesions in the thoracolumbar spine. These abnormalities are thought to represent chronic repetitive trauma to the vertebral ring apophysis of the lower thoracic and upper lumbar spine (Reprinted by Permission of SAGE Publications. Rachbauer et al. (2001): 447)
15.3 Snowboarding
15.3.1 Biomechanics of Snowboarding
As in skiing, there are numerous forms of snow-boarding, commonly divided into free riding (simply getting from the top of the slope to the bottom), alpine racing (e.g., slalom), and free-style (performing various trick maneuvers). These include jumping such as, big air where tricks are performed off a large jump, and half pipe where boarders descend a semicircular ditch from side to side and perform maneuvers while in the air above each side (American Association of Snowboard Instructors 2013).
Injuries tend to occur during the carving turns of a descent in alpine or free riding and during the landing of jumps and related tricks. The 2 principle snowboarding turns are the sliding turn (practiced predominately by beginners) and the carving turn with various combinations of the 2 in between. We will focus on the carving turn.
15.3.1.1 Board and Boot Design
A snowboard has features similar to a carving ski. It has a nose (leading end of the board), waist (determined by the side cut), and tail. Most boards have varying degrees of camber and torsional flexibility depending upon the materials from which they are manufactured. Designs vary depending upon their use, i.e., more rigid for alpine racing and more flexible for freestyle/trick maneuvers.
Snowboard boots tend to be classified as “soft shell” composed of non-rigid materials similar to a thick sports shoe used by most recreational snowboarders; “hard shell” composed of an outer casing of stiff plastic/composite materials with soft inner liners, similar to a ski boot used in alpine racing; and “hybrid” boots that combine various features to match individual preferences and requirements.
15.3.1.2 Carving Turns
Snowboarders descend much like skiers. A series of linked turns enable the snowboarder to reach the bottom of the slope. However, whereas a skier’s left side carving turn is essentially a mirror image of their right-sided turn, a snowboarder has to link two types of turns together as they traverse the fall line. They must coordinate balance, rotatory position, and control over edge angle, to adjust their center of gravity over alternating toe-side edge (plantar flexion) and heel-side edge (dorsiflexion) positions of the snowboard.
Another variable is an individual’s preference for foot position, which determines which side of the body leads down the slope. Most snowboarders lead with the left side (known as “regular” stance), while the rest lead with the right (“goofy”-footed stance). This is reflected in studies demonstrating that the limbs of the (left/regular) leading side of the body are more frequently (up to 40 %) injured in snowboarding (Bladin et al. 1993; Dohjima et al. 2001).
There is relatively little literature describing the biomechanics of a snowboarding turn. Various methods are used to achieve a turn among those of differing skill levels, and in practice analysis of a snowboard turn is extremely complex (Mallory 2011). This description is an attempt at a generic description of the snowboard carving turn using the aforementioned phases of the skiing turn.
Initiation phase (above the fall line): Body weight is transferred to the lead foot with ankle, knee, and hip flexion and the torso facing down the fall line, initiating downslope momentum.
Steering phase I (into the fall line): As the board drifts from a perpendicular position to align with the fall line, the knees and hips extend which returns a more even load distribution to the board (Delecluse et al. 2001) resulting in speed gain. Early edging is initiated.
Steering phase II (through the fall line): As speed increases, the center of gravity is again drawn forward with a return to hip and knee flexion, but the joint position and load differs between front-side and back-side turns. Toe-/front–side turns are achieved by increased ankle dorsiflexion, eversion, and external rotation (Delorme et al. 2005) (particularly of the backfoot) (Delorme 2004), slight knee flexion with hip/lumbar flexion (inclination) placing the center of gravity over the front working (toe) edge of the board to enhance balance and overcome centrifugal force of the turn.
Heel (back)-side turns require only slight plantar flexion during the midpoint of the turn, with varying degrees of eversion and external rotation. The nature of the turns dictates that less hip and lumbar flexion occurs and while the center of gravity remains over the working (heel) edge, weight is shifted more toward the rear foot (Dohjima et al. 2001).
It should be noted that the degree of motion in each plane of the ankle joint can be affected by the positioning of bindings (Woolman and McNair 2006) from relatively perpendicular (more common in freestyle) to more parallel (closer to skiing position for added speed in alpine snowboarding).
Unloading/edge changing phase: is similar to that of the unloading phase in skiing in that, as deceleration occurs, the torso and upper limbs (which had been counteracting the centripetal forces of the turn) return to a more upright and central position over the center of the board. There is also a relative reduction in knee, hip, and lumbar flexion in preparation to adjust position for the ensuing toe- or heel-side turn.
15.3.2 Lower Limb Snowboarding Injuries
Unlike skiing, lower limb snowboarding injuries (19–49 % of all injuries) are less frequent than those sustained by the upper limbs (Yamagami et al. 2004; Sakamoto and Sakuraba 2008). The ankle is the most commonly injured region of the lower limb, accounting for approximately 9 % of all injuries in adults (Moore and Knerl 2013).
Injury severity and location are influenced by the board rider’s skill level. Significantly higher proportions of injuries (including serious injuries) occur in the rider’s first snowboarding season (Bladin et al. 1993; O’Neill and McGlone 1999). Experienced or “elite”-level snowboarders sustain greater numbers of serious injuries and more lower extremity, head/face, and trunk injuries than less experienced riders. Beginners and novice riders experience a disproportionately higher rate of upper limb injuries (Wijdicks et al. 2014; Ogawa et al. 2010a).
15.3.2.1 Foot and Ankle Injuries
Ankle sprains are the most common ankle injury (52 %) compared to ankle fractures (44 %). Medial and lateral malleolar fractures constitute 64 % of all ankle injuries, and fractures of the talus account for 36 %. Of those, 95 % involve the lateral process of the talus (LPTF) (Kirkpatrick et al. 1998). Overall incidence of reported LPTF injuries is between 0.2 and 2.3 % (Moore and Knerl 2013; Wijdicks et al. 2014). It is a relatively rare injury outside snowboarding, accounting for less than 1 % of ankle fractures in one series, typically associated with high-velocity trauma such as a fall from a height or motor vehicle collisions (Mukherjee et al. 1974).
Mechanism
Retrospective reporting of lower limb injuries overwhelmingly includes falling as the predominant cause (75–91 %, 25 % associated with jumping), followed by twisting (12 %), and collisions (8 %) (Bladin et al. 1993; O’Neill and McGlone 1999). Injury mechanisms reported by Ogawa et al. included isolated falls at 49 %, jumping at 26 %, and collisions at 21 % (O’Neill and McGlone 1999). There is no correlation between reported mechanism and type of ankle injury. While the overall ankle injury rate does not appear to be affected by boot type, LPTF injuries appear to occur more commonly with hard shell boots (Wijdicks et al. 2014).
The pathomechanics of injuries of the LPTF is still being debated. Most authors feel that dorsiflexion is a necessary initial position, with eversion (Funk et al. 2003) (as opposed to inversion) and external rotation (Boon et al. 2001) implicated as essential components to induce the subtalar incongruity (Wijdicks et al. 2014) necessary for overload/fracture of the lateral process (Valderrabano et al. 2005).
Imaging
LPTF injuries are notoriously difficult to detect by plain radiographic assessment, especially if clinical information is scarce. Identification is important as delayed diagnosis and treatment is associated with poorer outcomes (Funk et al. 2003). A simple review of case series from the 1970s and 1980s suggests a false-negative rate of around 40 % on plain radiographs (Mills and Horne 1987). One would hope that an increasing awareness of this injury and better-quality radiographs would have improved this statistic. Ankle radiographs performed in plantargrade with 0 and 10–20° of internal rotation (Ogawa et al. 2010a) or 45° of internal rotation and 30° of plantar flexion (Dimon 1961) have been advocated to improve sensitivity (Fig. 15.7). Ultimately, as with any suspected injury to the tarsus, CT is the modality of choice to characterize the fracture size, extent of comminution, and articular involvement and to document any concomitant radiographically occult injuries (Fig. 15.8). MRI will demonstrate bone edema and soft tissue injuries not demonstrated on CT.


Fig. 15.7
A 19-year-old male snowboarder with a fracture of the lateral process of talus. The patient who sustained an eversion and external rotation injury after misjudging a jump landing. Plain radiograph of the left ankle demonstrates a subtle fracture of the lateral process of the talus (arrowhead)
Fig. 15.8
A 22-year-old female snowboarder with a fracture of the lateral process of talus. Coronal reformatted CT image of the ankle demonstrates an undisplaced comminuted fracture of the lateral talar process (arrowhead)
Ultrasonography has been described in the incidental diagnosis of LPTF injuries (Copercini et al. 2003) and may prove useful in cases where such injuries have not been previously identified and ultrasound assessment of capsuloligamentous and tendons has been requested.
15.3.2.2 Chronic Boot-Related Injuries
Repetitive friction superficial to the malleoli or adjacent to the top edge of a boot (typically new or ill fitting) results in irritative inflammation of the subcutaneous tissues and development of adventitial bursitis or “pseudotumor of the ankle.”
Imaging
Malleolar bursitis: Focal high T2/low T1 signal approaching that of fluid, superficial to a bony prominence with possible adjacent soft tissue and/or bone marrow edema, is demonstrated on MRI (Fig. 15.9). Occasionally the walls of these chronic bursae can rupture (Brown et al. 2000) which would alter T1 signal intensity depending on its acuity. Also, care must be taken to correlate imaging and clinical findings as occasionally a local breach in the skin can result in a septic bursitis which could initially have a similar imaging appearance.