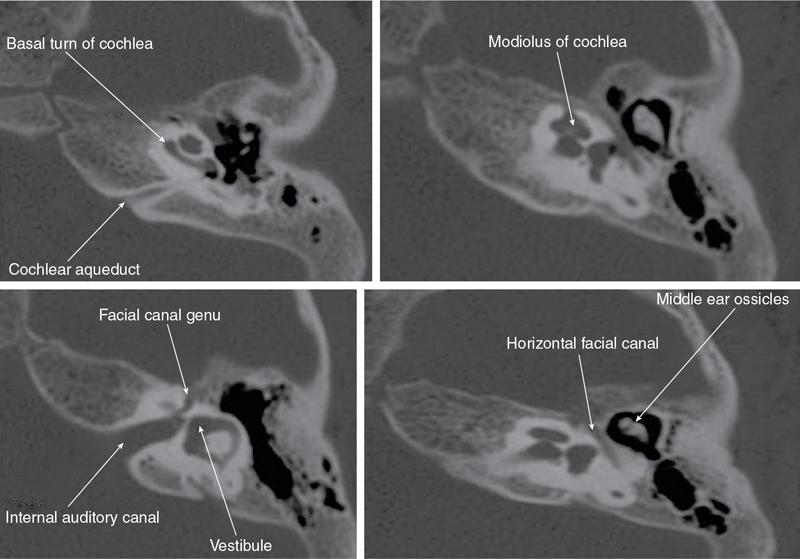
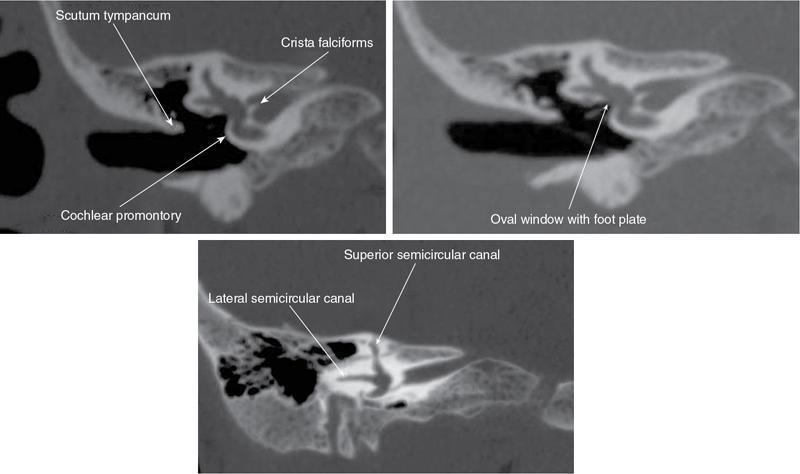
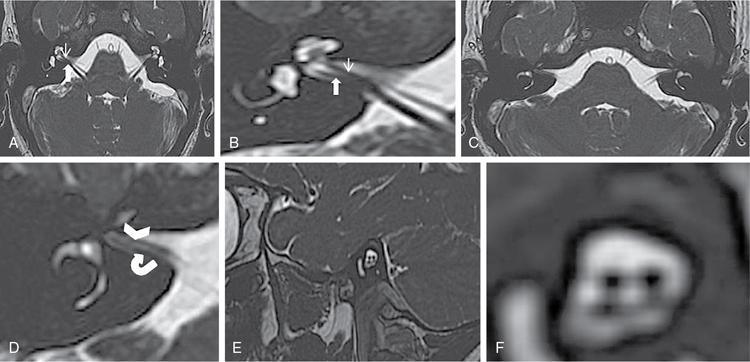
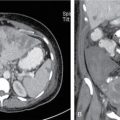
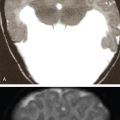
Rajendra Solanki, Poornima Digge, Gaurav Mutha, Pooja Prajapati HRCT (high-resolution CT scan) and high-field MRI are routinely performed imaging studies in paediatric patients with congenital hearing loss. CT and MRI are currently used for the evaluation of anatomical status of the cochlea and to become familiar with the normal anatomy of the inner ear and of the eighth cranial nerve. As the cochlear implant devices are currently being used more often for the treatment of patients with hearing loss, knowledge about the anatomy of the spiral canal of cochlea into which the electrode is placed has become paramount. In our study, we did both CT and MRI in all patients to review various common causes of congenital hearing loss. Bony labyrinth is well visualized in MDCT, while MRI is more helpful for membranous labyrinth. Vestibulocochlear nerve is well assessed on MRI particularly in parasagittal oblique plane & in axial plane. HRCT scanning is performed on 16-slice MDCT (GE) in the standard axial plane with helical technique (120 kV, 350 mA, pitch of 0.85, rotation time of 1 s, section thickness of 0.6 mm, matrix of 512 × 512). MR scanning is performed on 1.5 T GE, USA HDxt machine with following sequences. 3D FIESTA was performed with these parameters: 10-cm FOV, TR/TE of 8/4, 32 sections of 1-mm thickness, 256 × 256 matrix, flip angle of 45 degrees, bandwidth of ±32 kHz, two-phase cycles and an acquisition time of 2 min 24 s. FIESTA sequence in axial and parasagittal oblique is very important for the evaluation of the vestibulocochlear nerve. The cochlea is prone to a variety of congenital anomalies, depending on the exact time at which an insult occurs during embryogenesis. Terminology is often used imprecisely leading to confusion among clinicians. A classification first proposed in 1987 by Jackler et al. has become widely accepted (with various modification), which divides congenital cochlear anomalies according to the timing of developmental arrest. Conveniently starting from the third week of gestation, an insult during each subsequent week results in a distinct inner ear abnormality. Fig. 3.34.1A and B depicts the normal anatomy for reference to understand the further text. MRI is superior in assessing the patency of membranous labyrinth, detected even smaller spiral canal sclerosis and obstruction. It is easy to put proper size electrode array after 3D CT and 3D MRI. Postprocessing 3D reconstruction with advanced software will help in the detail evaluation of cochlear turns, semicircular canals defect and dilated endolymphatic duct and sac. MDCT also provides the superb colour-coded volume-rendering images in patients with postcochlear implantation study to know the exact location of active electrode in cochlea, which is never possible with conventional CT scan study. MRI study is contraindicated in postcochlear implantation patient due to electromagnetic property of active electrode (Figs 3.34.2 and 3.34.3).
3.34: Implant pre and post-surgical imaging
Technical parameters in CT scan and MRI
Cochlea
Cochlear Deformities
Gestational Age at Arrest (weeks)
Frequency
Michel deformity
Third
Very rare
Common cavity
Between fourth and fifth
25%
Cochlear aplasia
Fifth
Uncommon
Cochlear hypoplasia
Six
15%
IP-I (incomplete partition type I)
Between sixth and seventh
Uncommon pseudo-Mondini
IP-II (incomplete partition type II)
Seventh
55% Classic Mondini
Normal anatomy
This is discussed in detail in chapter on internal ear (Chapter 3.33)
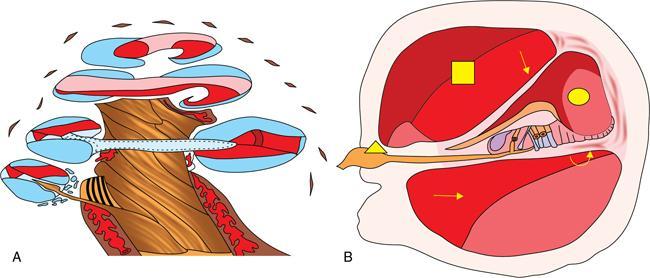
 ), scala tympani (
), scala tympani (  ), cochlear duct (
), cochlear duct (  ), basilar membrane (
), basilar membrane (  ), Reissner’s membrane as well as cochlear nerve (
), Reissner’s membrane as well as cochlear nerve (  ).
).
Anomalies of cochlea
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


