8 | Indications for Obstetric Ultrasound |
In what follows we will discuss the indications for the use of Doppler ultrasound in obstetrics. We recommend the use of Doppler ultrasound in obstetrics under the following circumstances, usually in the second half of pregnancy, except when malformations are suspected:
1. Suspected intrauterine growth restriction (IUGR),
2. Pregnancy-induced hypertension (PIH), preeclampsia, eclampsia,
3. Status post dysmature delivery/intrauterine death,
4. Status post preeclampsia/eclampsia,
5. Abnormalities in the recorded fetal heart rate,
6. Reasonable suspicion of fetal anomalies or fetal disease,
7. Multiple pregnancy with discordant growth,
8. Suspicion of cardiac anomalies or heart disease.
Before discussing each of these indications in detail, we must consider the diagnostic capabilities of ultrasound in principle. In the first place Doppler ultrasound can display blood flow and its direction in a blood vessel (color Doppler), and under certain conditions estimate blood flow velocity in these vessels. This information can be used to diagnose malformations, especially cardiac anomalies. Secondly, the degree of resistance in a vascular segment can be ascertained. This information is used to determine the condition of the fetus, especially in the third trimester. Changes in the resistance of fetal vessels correlate with various findings in the infant. Imminent danger to the infant may be deduced from a redistribution of the blood from the periphery to vital organs. Unremarkable resistance readings indicate that the infant’s nutrition is balanced, while abnormal values suggest poor nutritional supply, to which the infant responds with redistribution of its blood supply.
When placental insufficiency is compensated it is intrinsically possible for normal Doppler values to be recorded, showing a balanced supply, while abnormal Doppler values always expose decompensation. Because of this fact it is not possible to screen for placental insufficiency with the use of Doppler ultrasound. Rather, it is used to clarify the significance of a placental insufficiency demonstrated most often by biological measurements.
Thus, Doppler ultrasound makes it possible to distinguish between a compensated and a decompensated placental insufficiency. This is its most important task. Doppler ultrasound can also contribute more, but not less, to the evaluation of the condition of the fetus.
Note also that in fetal diagnosis Doppler ultrasound as a rule only recognizes chronic conditions, not acute changes, i.e., it primarily helps in the detection of chronic placental insufficiency. Cases have been recorded in which acute abruption of the placenta was not detected when Doppler ultrasound happened to be used coincidentally, since the lack of blood flow in the affected area is not accessible to the Doppler, while blood flow in the remaining placenta is unchanged. Moreover, Doppler ultrasound could not predict acute placental insufficiency, only the risk associated with chronic placental insufficiency. Clearly Doppler ultrasound is not suited to examining transmitted diseases, since these first and foremost threaten acute placental insufficiency.
The obstetric indications for Doppler ultrasound listed above primarily address two situations:
– Firstly, the diagnosis and further evaluation of malformations, as a rule by color Doppler. Doppler ultrasound is used principally to show the anatomy.
– Secondly, the diagnosis and surveillance of a high-risk pregnancy toward the end of the second trimester and in the third trimester. The main problem addressed is growth restriction of the fetus, i.e., diagnostic surveillance of the condition of the fetus.
Doppler ultrasound is used in the diagnosis of anomalies to display the anatomy and, at times, the function of the organs. As a rule this requires color Doppler ultrasound. For instance, in fetal cardiac anomalies color Doppler sonography can demonstrate the cardiac defect and, by displaying the direction of flow, allow conclusions about their functional significance.
Determining the condition of the fetus in the third trimester primarily requires an analysis of the waveform. Color display of the vessels serves at best to find and display the course of the vessel.
The most important indication for monitoring the condition of the fetus in the third trimester is fetal IUGR. This suggests that the most important basis for the use of Doppler ultrasound is biological measurement. Exclusion of malformations is another strict indication for the introduction of Doppler ultrasound. This can be justified by the fact that in growth-restricted infants malformations are seen significantly more commonly than in eutrophic infants. Infants with chromosomal aberrations are also often growth restricted.
IUGR and Biological Measurement
Since growth restriction is the most important indication for Doppler ultrasound this section will briefly review those measurements leading to the diagnosis.
The fundamental biological measurement is the exact gestational age. To determine this, the sonographic measurement of crown–rump length is indispensable. The sooner this measurement is made, the more precise is the determination of gestational age.
Basic Principles
Biological measurements primarily serve to recognize disturbances in intrauterine growth. Reference planes (Figs. 8.1, 8.2) must be determined precisely in order to make results reproducible and comparable. A single measurement is not enough, as it can easily lead to misinterpretation. For instance, biparietal measurements in a dolichocephalic skull may create doubt because they are too small.
Biological measurements are also a window into the diagnosis of malformations. If the positional plane cannot be displayed or if measured values deviate significantly, the cause of the problem must be sought by a thoroughgoing ultrasound examination.
The literature provides a variety of measuring techniques. In what follows we confine ourselves to what we consider to be those most commonly employed.
Some Specific Measurements
Skull
![]() Measurements of the skull include the biparietal diameter (BPD), the occipitofrontal diameter (OFD), and the head circumference (HC) (Fig. 8.1).
Measurements of the skull include the biparietal diameter (BPD), the occipitofrontal diameter (OFD), and the head circumference (HC) (Fig. 8.1).
 The reference plane is set correctly when the infantile head appears oval with bony structures throughout. The middle echo should be interrupted by the cave of the septum pellucidum in the anterior third of the skull.
The reference plane is set correctly when the infantile head appears oval with bony structures throughout. The middle echo should be interrupted by the cave of the septum pellucidum in the anterior third of the skull.
 If the cerebellum or the orbits are seen, the plane is too occipital or caudal.
If the cerebellum or the orbits are seen, the plane is too occipital or caudal.
Abdomen
 The abdominal diameter (AD), antero–posterior diameter, and circumference are determined (Fig. 8.2).
The abdominal diameter (AD), antero–posterior diameter, and circumference are determined (Fig. 8.2).
 The two diameters are identical in the ideal rounded form of the abdomen.
The two diameters are identical in the ideal rounded form of the abdomen.
 In the correct measuring plane the dorsal third of the umbilical v. can be seen. The sections of the ribs must be symmetrical. In addition, the three ossification centers of the vertebral column must be visible.
In the correct measuring plane the dorsal third of the umbilical v. can be seen. The sections of the ribs must be symmetrical. In addition, the three ossification centers of the vertebral column must be visible.
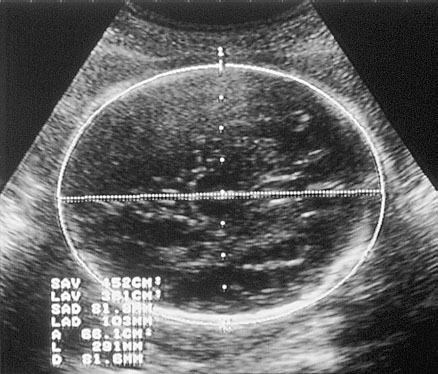
Fig. 8.1 Ultrasound scan of head. 1. Thalamic nuclei, 2. Cave of septum pellucidum. Measurements displayed include the BPD, the OFD, and the HC.
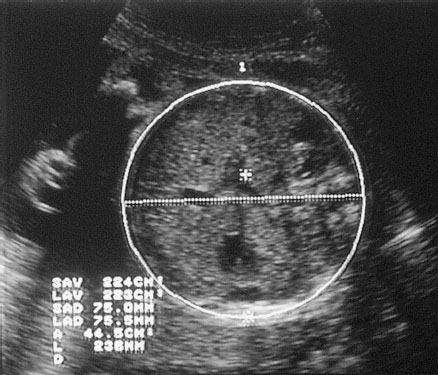
Fig. 8.2 Ultrasound scan of abdomen. 1. Umbilical vein, 2. Cross section of aorta, 3. Vertebral column. Measurements displayed include abdominal diameter and circumference.
 Care must be taken not to distort the abdomen by compression with the scanner or by respiratory movements.
Care must be taken not to distort the abdomen by compression with the scanner or by respiratory movements.
Extremities
 Measurement of the femoral diaphysis is now part of a routine diagnostic study (Fig. 8.3). It is only necessary to measure other long bones if the length of the femur deviates significantly or if its shape shows noticeable changes (Fig. 8.4).
Measurement of the femoral diaphysis is now part of a routine diagnostic study (Fig. 8.3). It is only necessary to measure other long bones if the length of the femur deviates significantly or if its shape shows noticeable changes (Fig. 8.4).
 The femur should be measured at a right angle to the direction of the sonic beam. If the two femurs run parallel to each other, measurement of the one closer to the transducer is preferred, because the measurement of the femur more distant from the transducer tends to be too short. The distance measured is identical to the ossified part of the bone without consideration of any curvature that may be present.
The femur should be measured at a right angle to the direction of the sonic beam. If the two femurs run parallel to each other, measurement of the one closer to the transducer is preferred, because the measurement of the femur more distant from the transducer tends to be too short. The distance measured is identical to the ossified part of the bone without consideration of any curvature that may be present.
Related posts:
 Diagnosis of the Uterine Tube by Transvaginal Sonography
Diagnosis of the Uterine Tube by Transvaginal Sonography
 Doppler Sonography in Obstetrics—Screening At-Risk Populations
Doppler Sonography in Obstetrics—Screening At-Risk Populations
 Doppler Ultrasound and the Cardiotocogram
Doppler Ultrasound and the Cardiotocogram
 Doppler Ultrasound in the Diagnosis of Fetal Anomalies
Doppler Ultrasound in the Diagnosis of Fetal Anomalies
 Diagnostic Sonography of Blood Flow in Breast Tumors
Diagnostic Sonography of Blood Flow in Breast Tumors
 Vascular Supply of the Uteroplacentofetal Unit and Techniques for the Examination of Individual Vessels
Vascular Supply of the Uteroplacentofetal Unit and Techniques for the Examination of Individual Vessels
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


