Infections and Inflammations of Bones
Lee F. Rogers
Martha A. Norris
L. F. Rogers: Department of Radiology, Wake Forest University School of Medicine, Winston-Salem, North Carolina 27157. M. A. Norris: Department of Radiology, University of Wisconsin Hospital and Clinics, Madison, Wisconsin 53792-3252.
OSTEOMYELITIS
Osteomyelitis was once a common, devastating, often crippling, and much-feared disease. Since the advent of antibiotics, it has become manageable, less common, and much less serious. The general improvement in personal hygiene, greatly improved surgical antisepsis, and early antibiotic treatment of lesions that predispose to septicemia have resulted in an appreciable reduction in the incidence of osteomyelitis.
Infections of bone have been conveniently divided into three categories reflecting the source of the infection14: (1) hematogenous osteomyelitis; (2) implantation osteomyelitis caused by bacteria implanted or introduced with an open fracture, penetrating wound, or surgical procedure; and (3) secondary osteomyelitis with the bone involvement secondary to a contiguous focus of soft-tissue infection related to peripheral vascular disease. Osteomyelitis may also be divided into acute, subacute, and chronic forms, depending on the virulence of the organism, the response of the host, and the effectiveness of antibiotic treatment.
Staphylococcus aureus is the offending organism most frequently identified. In children, in whom hematogenous infection is the rule, multiple foci of disease are relatively common, whereas in adults the infection is usually limited to a single focus. The cause is usually established by obtaining a positive blood culture, a culture from an aspiration of the adjacent joint, or a direct aspiration of the involved bone or overlying soft tissues. Early recognition and treatment with antibiotics may minimize the radiographic findings of osteomyelitis.
Pathogenesis
Hematogenous Osteomyelitis
The source of bacteria in the hematogenous form is usually infections of the skin, boils or carbuncles, insect bites, infected abrasions, or, less commonly, infections of the respiratory tract. The offending organism is usually S. aureus, less commonly Streptococcus, Haemophilus influenzae, or pneumococcus. The organisms enter the bloodstream and become entrapped in the terminal vascular networks of long bones, the site and consequences depending on the age of the patient (Fig. 5-1). In childhood, these networks are located in the metaphysis just beneath the physis, and therefore the infections of childhood are most often located in and limited to the metaphyseal ends of long bones, particularly the femur and tibia14,21 (see Figs. 5-4 and 5-5). Involvement of adjacent joints is rare. Terminal vascular networks are also located in the epiphysis, but isolated infections of the epiphysis are much less common than those in the metaphysis.17 In contrast, in infants younger than 1 year of age, the vascular network commonly crosses the growth plate from the metaphysis to the epiphysis; therefore, infections in infancy are more likely to originate within the epiphysis or to extend quickly from the metaphysis into the epiphysis and then into the adjacent joint.14,21 Extension of the infection into the adjacent joint is much less likely after the age of 1½ years, except in the hip, where the metaphysis is located within the joint capsule. After the closure of the epiphysis, the terminal blood supply is located in the end of the bone. Therefore, in adults, the hematogenous infections occur at the end of the bone and may extend into the adjacent joint space. However, primary hematogenous osteomyelitis of long bones is uncommon in adults. Adults are more likely to have vertebral osteomyelitis or suppurative spondylitis, often secondary to infection or manipulation of the urinary tract.
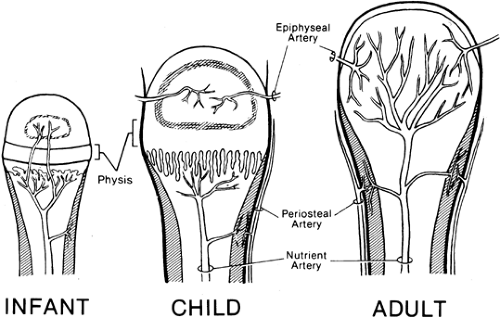 FIG. 5-1. Vascular supply of bone. The principal blood supply to the end of bone is from the nutrient artery in the medullary canal. In the infant and until 18 months of age, small vessels perforate the physis to enter the epiphysis. After 18 months of age, the vascular supply assumes the pattern of childhood and the perforating vessels involute. The epiphysis and metaphysis then have separate blood supplies. In the adult, after closure of the physis, the branches of the nutrient artery extend to the end of bone. Note the blood supply to the cortex. Branches of the periosteal artery supply the outer cortex, whereas branches of the nutrient artery supply the inner cortex. |
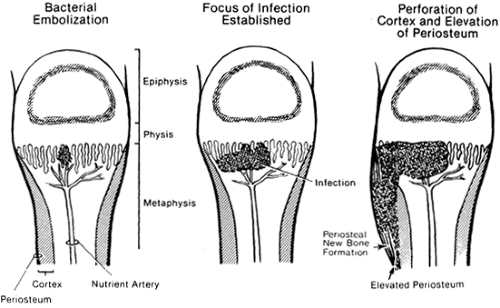 FIG. 5-2. Pathomechanics of hematogenous osteomyelitis. Bacterial embolization occurs through the nutrient artery, and bacteria lodge in the terminal blood supply in the metaphysis. After the infection is established, it expands within the medullary canal toward the cortex and the diaphysis. The physis is an effective barrier. The infection then extends through the vascular channels in the cortex to elevate and strip the periosteum from the cortex. Periosteal new-bone formation occurs. Note that the bond between the periosteum and the perichondrium at the physis prevents extension of the infection into the joint. |
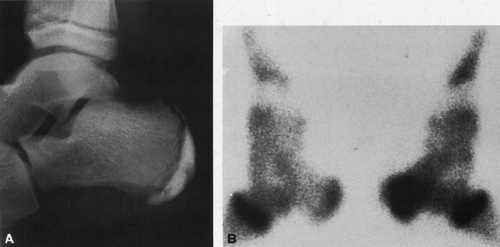 FIG. 5-3. Acute osteomyelitis of the left calcaneus in a child. A: Lateral radiograph demonstrates no bony abnormality. Deep soft-tissue swelling is present adjacent to the posterior and inferior surfaces of the calcaneus. B: Technetium-99m bone scan reveals focus of increased activity in the left calcaneus. Bilateral increased activity at the distal tibial epiphysis is normal. (Courtesy of James Conway, M.D., Chicago, Illinois.) |
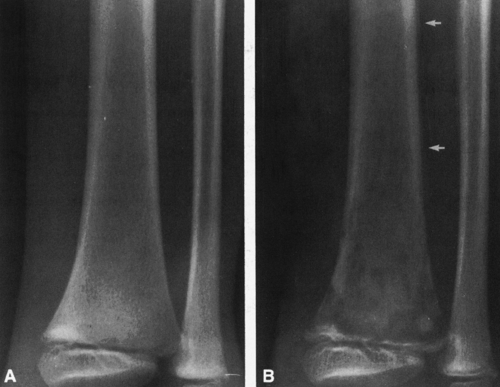 FIG. 5-4. Acute osteomyelitis in the distal tibia. A: The bone is completely normal; however, edema and soft-tissue swelling are present adjacent to the medial surface of the tibia, with obliteration of portions of the subcutaneous fat. This is the earliest radiographic sign of osteomyelitis. B: Repeat examination obtained in 11 days demonstrates irregular permeative and mottled destruction within the metaphysis, with a perforation and destruction of the cortex in several areas. Periosteal elevation is identified proximally (arrows). |
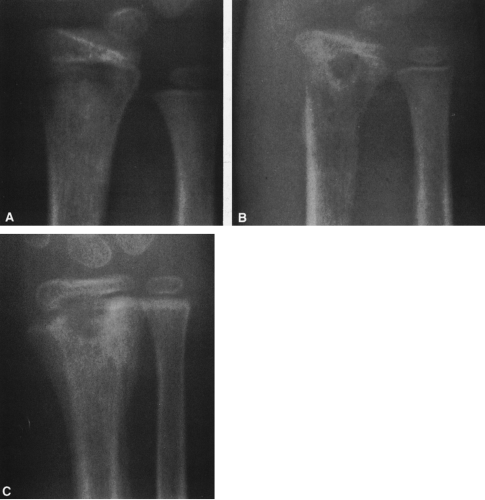 FIG. 5-5. Acute osteomyelitis of the distal radius. A: Initial examination demonstrates irregular lysis and destruction in the distal metaphysis. The epiphysis remains intact. B: Repeat examination in 9 days demonstrates obvious destruction, which now extends proximally toward the diaphysis. Cortical destruction and considerable overlying soft-tissue swelling are present. Note the periosteal new-bone formation. C: Eight-week follow-up examination. Healing is demonstrated by the compact periosteal reaction filling in a portion of previously destroyed bone. Note that the process did not extend into the epiphysis. |
The infectious process begins in the intramedullary portion of the bone, eventually leading to the destruction
of the trabeculae, penetration of the overlying cortex through vascular foramina, elevation of the periosteum, and extension into the overlying soft tissues (Fig. 5-2).
of the trabeculae, penetration of the overlying cortex through vascular foramina, elevation of the periosteum, and extension into the overlying soft tissues (Fig. 5-2).
The periosteum is easily elevated by the extension of pus through the cortex. Because the periosteum is tightly bound to the perichondrium of the physis or growth plate, the periosteum is preferentially stripped or elevated from the metaphysis toward the diaphysis, often well beyond the extent of involvement of the intramedullary bone or marrow. The tight bond between the periosteum and perichondrium at the physis prevents extension of pus into the epiphysis or adjacent joint except at the hip, where the metaphysis lies within the joint. In contrast to that in children, the periosteum in adults is tightly adherent to the cortex and much less easily stripped. Therefore, in adults, periosteal elevation is not as marked, the extent of periosteal stripping is more limited, and involucrum formation is uncommon.
Implantation Osteomyelitis
Implantation osteomyelitis is caused by bacteria introduced into the soft tissues and bone by a penetrating wound, surgical procedure, or open fractures and dislocations (see Fig. 5-8). Blood clot, necrotic marrow, muscle, and other soft tissues provide an excellent culture medium for the localization and colonization of pathogenic bacteria. S. aureus is a common offending organism, but other gram-positive organisms such as Streptococcus and gram-negative organisms such as Pseudomonas, Proteus, or Escherichia coli may be involved.
 FIG. 5-6. Acute osteomyelitis of the ulna. A: Examination obtained 10 days after the onset of symptoms demonstrates permeative destruction of most of the ulna, with periosteal new-bone formation surrounding the distal shaft and metaphysis. B: Repeat examination 1 week later shows an increase in the amount of subperiosteal new-bone formation. C: Examination 6 months later shows residual cortical thickening but no definite areas of bone destruction. |
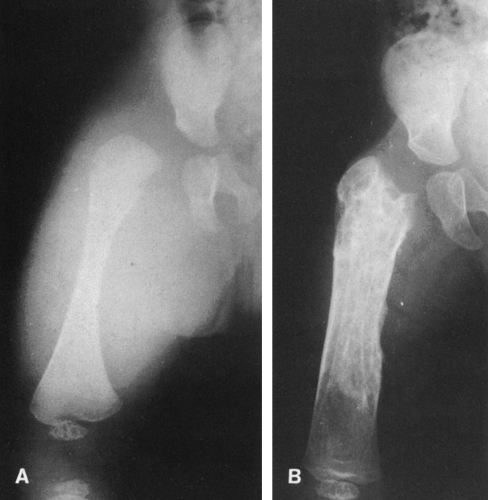 FIG. 5-7. Acute osteomyelitis of the femur associated with suppurative arthritis of the hip in an infant. A: Examination 7 days after the onset of fever and swelling of the thigh. Note the massive soft-tissue swelling and lateral dislocation of the femur, indicating an associated joint effusion. Minimal cortical destruction is evident in the medial aspect of the metaphysis. B: Examination obtained 3 months later shows extensive new-bone formation surrounding much of the shaft. Remnants of the old shaft are visible. Several rounded or oval radiolucencies are seen in the proximal femur, possibly representing residual foci of infection. The hip joint is no longer dislocated. |
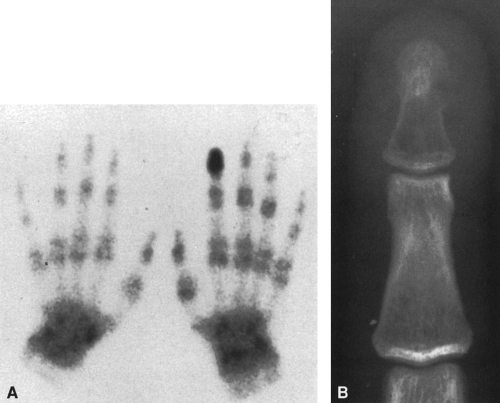 FIG. 5-8. Human bite with osteomyelitis. This man sustained a human bite on the tip of the index finger 2 weeks previously. He presented with obvious swelling and redness over the distal phalanx. The clinical question was to distinguish between cellulitis and osteomyelitis. A: Technetium-99m bone scan, 2-hour delay, demonstrates increased activity in the distal phalanx. B: Anteroposterior radiograph demonstrates a breach in the lateral cortex just beneath the ungual tuft and a hollowing or shelling out of the trabeculae in the distal phalanx. There is no periosteal reaction. Findings are indicative of osteomyelitis. |
Secondary Osteomyelitis
Osteomyelitis associated with vascular insufficiency is almost always encountered in the diabetic patient and localized to the foot, affecting the phalanges and metatarsals (see Fig. 5-16). Infection of bone is always secondary to an overlying cellulitis or deep penetrating ulcer of the skin. The most common offending organism is S. aureus or Streptococcus, although gram-negative bacterial infections are also encountered.
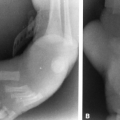
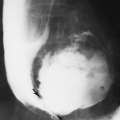
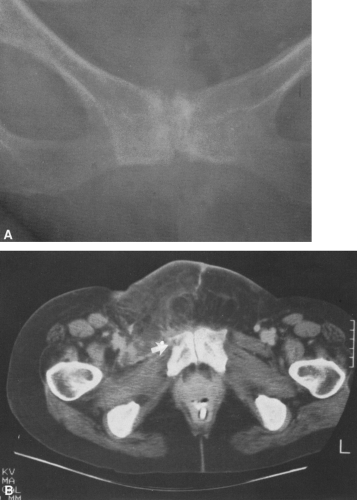 FIG. 5-9. Osteomyelitis of the right pubic bone. A: On the anteroposterior view there is no definite abnormality. B: Computed tomographic scan demonstrates extensive soft-tissue changes anterior to the pubis and a break in the cortex (arrow) consistent with osteomyelitis and overlying cellulitis. |
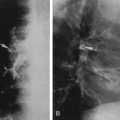
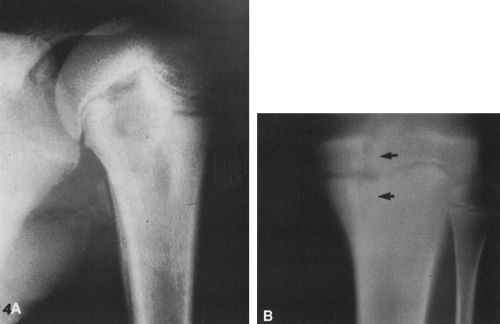 FIG. 5-10. Two cases of subacute bone abscess in children. A: An elongated radiolucency in the proximal humerus, surrounded by sclerosis with overlying periosteal new-bone formation, extends for some distance down the humeral shaft. Proximally, it abuts the growth plate. B: Serpiginous lucency in the proximal metaphysis of the tibia extends across the growth plate into the epiphysis (arrows). Note that it is marginated by a fine sclerotic rim. (Courtesy of Andrew K. Poznanski, M.D., Chicago, Illinois.) |
 FIG. 5-11. Chronic bone abscess, or Brodie’s abscess. A: The abscess cavity is seen as a well-demarcated area of radiolucency surrounded by sclerotic bone. The overlying cortex is thickened by compact periosteal new-bone formation. B: Chronic bone abscess of the proximal humerus. A rounded radiolucency is surrounded by a relatively thickened wall of sclerosis. Periosteal new-bone formation is present in the metaphysis. |
 FIG. 5-12. Chronic osteomyelitis. The entire radius is involved. There are irregular cavities representing chronic abscesses, and a large, dense sequestrum surrounded by involucrum is noted within the cavity in the distal end of the shaft. The original cortex has been completely replaced. |
 FIG. 5-13. Chronic osteomyelitis. Cortical thickening and sclerosis involve the entire shaft, particularly distally. Some ovoid radiolucencies can be seen within the thickening. |
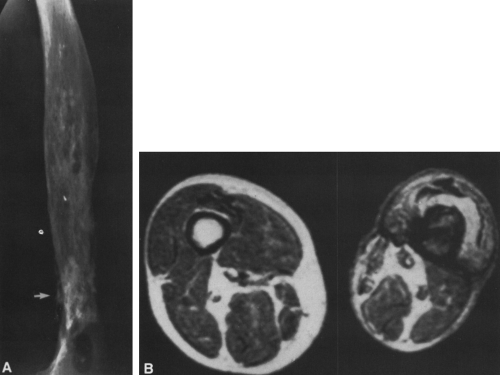 FIG. 5-14. Chronic osteomyelitis of the femur, with intermittent drainage over a period of 40 years. A: The cortex has expanded. Irregular patches of sclerosis and lucency are present throughout the diaphysis. A large radiolucency is present distally. Periosteal new-bone formation is present (arrow). B: T1-weighted magnetic resonance image. Note the obvious atrophy of the involved extremity. The cortex is poorly defined and is expanded and thin. The intramedullary cavity has a low signal compared with the opposite side, indicative of persistent infection. |
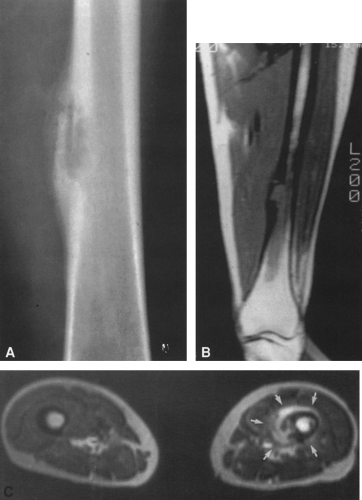 FIG. 5-15. Cortical abscess of the midfemoral shaft in an intravenous drug abuser. A: Anteroposterior view demonstrates considerable linear and nodular (sometimes known as lamellonodular) periosteal reaction overlying a lucent lytic defect in the medial cortex. This type of periosteal reaction is usually indicative of infection. B: Coronal T1-weighted magnetic resonance image demonstrates low signal within the marrow surrounding the lesion in the medial cortex. The overlying soft-tissue mass is not sharply defined. C: T2-weighted axial image. This image demonstrates a high signal from the surrounding soft-tissue mass surrounding the lesion and cortex (arrows). Note that the signal emanating from the intramedullary space is higher than that of the normal bone marrow on the opposite side. This is indicative of active infection. The cortical abnormality is well demonstrated. (Courtesy of Alfred L. Horowitz, M.D., Chicago, Illinois.) |
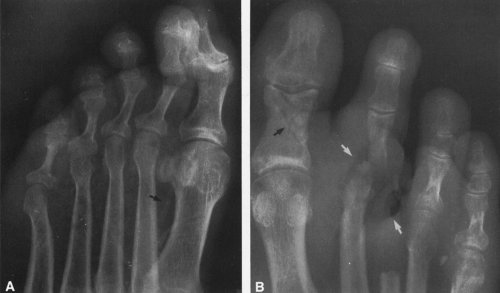 FIG. 5-16. Infections in the diabetic foot. A: Multiple small radiolucencies are present within the soft tissues of the foot underlying the metatarsals, identifying the site of a soft-tissue infection. No bony abnormalities are present, and therefore there is no radiographic evidence of osteomyelitis. Note the arterial calcification (arrow), indicative of diabetes. B: An amputation of the third toe was performed previously. A large collection of air (white arrows) identifies the site of an ulcer on the plantar surface of the foot. Note the lytic destruction of the apposing surfaces of the second metatarsophalangeal joint, with associated subluxation indicative of osteomyelitis and suppurative arthritis. Closer examination also reveals lytic destruction of the medial side of the head of the fourth metatarsal. There is also a fracture of the proximal phalanx of the great toe (black arrow) without a history of trauma, indicative of neurotrophic arthropathy. |
Infections of bone are discussed in this chapter. Infections of joints and infectious spondylitis are detailed in Chapter 3.
RADIOGRAPHIC FINDINGS IN ACUTE OSTEOMYELITIS
In acute osteomyelitis there is a latent period of 10 to 12 days between the time of onset of clinical symptoms and the development of definite radiographic changes in bone.14 Because it is essential that adequate therapy be instituted as early as possible, one should not wait for the development of radiographic evidence of disease before instituting appropriate treatment. Radioisotopic bone scanning is very sensitive to the changes of osteomyelitis, revealing areas of increased radioactivity at sites of infection well before there is any plain film radiographic sign of disease (Fig. 5-3). A bone scan is warranted in every case of clinically suspected osteomyelitis in which the radiographs are unrevealing.
The first radiographic evidence of disease is the swelling of soft tissues, characteristically deep and adjacent to bone (Fig. 5-4; see Fig. 5-3A). The early swelling is recognized
because of displacement or obliteration of the normal fat planes adjacent to and beneath the deep muscle bundles. At first the superficial fatty layer is unaffected. In contrast, with skin infection, soft-tissue swelling is superficial and does not involve the deeper tissues adjacent to the bone. The first evidence of disease in the bone is usually an area of indefinite rarefaction or destruction in the metaphysis (Figs. 5-5 and 5-6). The area of destruction is poorly defined and has a fine, granular, or slightly mottled appearance. Associated with this or even at times preceding it is a minimal amount of periosteal new-bone formation laid down parallel to the outer margin of the cortex. The limits of the bone destruction remain poorly defined throughout the acute stage. The actual disease process is usually much more extensive than demonstrated by the radiograph.
because of displacement or obliteration of the normal fat planes adjacent to and beneath the deep muscle bundles. At first the superficial fatty layer is unaffected. In contrast, with skin infection, soft-tissue swelling is superficial and does not involve the deeper tissues adjacent to the bone. The first evidence of disease in the bone is usually an area of indefinite rarefaction or destruction in the metaphysis (Figs. 5-5 and 5-6). The area of destruction is poorly defined and has a fine, granular, or slightly mottled appearance. Associated with this or even at times preceding it is a minimal amount of periosteal new-bone formation laid down parallel to the outer margin of the cortex. The limits of the bone destruction remain poorly defined throughout the acute stage. The actual disease process is usually much more extensive than demonstrated by the radiograph.
In a short time, bone destruction becomes more prominent, causing a ragged, moth-eaten appearance of the medullary bone, with foci of destruction intermingled with areas of apparently more or less normal bone. Periosteal new-bone formation is more pronounced, and both the periosteal reaction and intramedullary destruction extend into the diaphysis (see Fig. 5-6). In the neonate, the infection commonly extends to the overlying joint, forming a suppurative arthritis (Fig. 5-7; see Figs. 3-5 and 3-6).
In the phalanges and other small bones there is little or no periosteal reaction. Bone is simply dissolved (see Fig. 5-16).
At times this proceeds internally, hollowing or shelling out the bone by destroying intramedullary trabeculae, leaving only a thin rim of cortex (Fig. 5-8).
At times this proceeds internally, hollowing or shelling out the bone by destroying intramedullary trabeculae, leaving only a thin rim of cortex (Fig. 5-8).
Radioisotopic Bone Scanning
Technetium-99m radiophosphate (see Figs. 5-3 and 5-8), gallium-67 citrate, and indium-111 leukocytes have been used to diagnose osteomyelitis and to differentiate osseous infections from those limited to the soft tissues (e.g., cellulitis).15,16 To distinguish skeletal from soft-tissue infection, a triple-phase 99mTc radiophosphate scan is performed (see Fig. 5-17). The three phases are perfusion, blood pool, and delayed images. Acute osteomyelitis is characterized by enhanced activity in the blood pool and delayed bone images, whereas septic arthritis and cellulitis demonstrate increased activity in the blood pool phase but normal or only slightly increased uptake in the delayed image. Sequential radiophosphate and gallium scanning may also be used, because increased radiophosphate uptake is nonspecific, occurring in areas of high bone turnover from whatever cause—fracture, infection, metabolic, or tumor. Gallium-67 uptake is more specific for infection. Indium-111 leukocytes deposit wherever there is an active migration of white cells, and therefore this examination is also more specific for infection.16
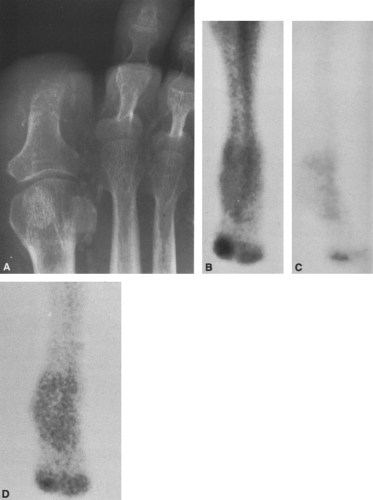 FIG. 5-17. Diabetic patient with soft-tissue infection. The ungual tuft of the great toe was previously amputated for osteomyelitis. There is now evidence of skin infection and a question of recurrent osteomyelitis. A: Vascular calcification is present. The margin of the amputation of the distal phalanx of the great toe is poorly defined. B and C: Two views from a three-phase technetium-99m bone scan. The immediate static image (B) shows increased activity in the region of the great toe, and this is diminished on the 2-hour delayed film (C), suggesting that the infection is a cellulitis without osteomyelitis. D: A gallium-67 scan was obtained for confirmation. The activity is no greater than that on the delayed 99mTc scan and confirms the absence of osteomyelitis. |
Computed Tomography
Computed tomography (CT) is a useful adjunct in the evaluation of osteomyelitis.5,7 Increased attenuation occurs within the bone marrow early in the disease, before plain film changes and simultaneously with increased radioisotopic activity. The increased attenuation is caused by the presence of edema and pus, which replaces the fat within the marrow. The attenuation of normal marrow fat is on the order of −80 to −100 Hounsfield units, increasing in
the presence of an infection to −10 Hounsfield units or higher, well within the positive range. This is similar in appearance to infiltration by tumors (see Fig. 4-43 in Chapter 4). Small bubbles of intraosseous gas may be seen within the intramedullary canal as a result of infection by gas-forming organisms. CT demonstrates to good advantage cortical destruction and associated soft-tissue changes (Fig. 5-9). Fat-fluid (pus) levels have been reported to occur within the medullary canal and adjacent bursae. CT is also advantageous in the evaluation of chronic osteomyelitis,5 allowing the detection and localization of bony sequestra, the demonstration of cortical defects leading to subcutaneous sinus tracts, and the identification of adjacent soft-tissue abscesses. Abscesses appear as sharply defined areas of low density within surrounding muscle or subcutaneous tissue.
the presence of an infection to −10 Hounsfield units or higher, well within the positive range. This is similar in appearance to infiltration by tumors (see Fig. 4-43 in Chapter 4). Small bubbles of intraosseous gas may be seen within the intramedullary canal as a result of infection by gas-forming organisms. CT demonstrates to good advantage cortical destruction and associated soft-tissue changes (Fig. 5-9). Fat-fluid (pus) levels have been reported to occur within the medullary canal and adjacent bursae. CT is also advantageous in the evaluation of chronic osteomyelitis,5 allowing the detection and localization of bony sequestra, the demonstration of cortical defects leading to subcutaneous sinus tracts, and the identification of adjacent soft-tissue abscesses. Abscesses appear as sharply defined areas of low density within surrounding muscle or subcutaneous tissue.
Magnetic Resonance Imaging
Magnetic resonance imaging (MRI) has proved to be more sensitive than standard radiography, conventional tomography, or CT in the evaluation of osteomyelitis.3




Related posts:



Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
