 Introduction
Introduction Congenital and Perinatal Infections
Congenital and Perinatal InfectionsTable 11-1 Selected Congenital and Perinatal Infections | |||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||
studies can show thrombocytopenia, direct hyperbilirubinemia, and elevated serum transaminases (16). The majority of infants with congenital CMV disease have permanent neurodevelopmental sequelae, including microcephaly, cerebral palsy, cognitive impairment, sensorineural hearing loss, visual abnormalities, and seizures. Sensorineural hearing loss can progress after birth, in both infants with congenital CMV disease and those who were without symptoms at birth (17). By contrast, the vast majority of CMV-infected infants who lack signs of infection, either at birth or subsequently, have normal neurodevelopmental outcomes. Steinlin et al. (18) have described a characteristic clinical syndrome in patients who are infected with CMV during the third trimester. Characteristics of the syndrome include microcephaly with sensorineural hearing loss, hyperactivity and associated behavioral problems, reduced apprehension for pain, and, sometimes, ataxia and hypotonia.
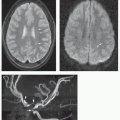
 Figure 11-1 Fetal congenital CMV infection. Twenty-eight weeks of gestation. A. Axial T2-weighted fetal MRI image shows bilateral periventricular germinolytic cysts (arrowheads) and abnormal gyri (arrows). B. Coronal T2-weighted image demonstrates diffuse polymicrogyria (arrows). (Courtesy of Catherine Adamsbaum, MD, Paris, France.) |
|
described in children with trisomy 13, trisomy 21, prenatal drug exposure, congenital heart disease, and a variety of anoxic and toxic injuries to the developing brain (31,32). Postmortem studies have described evidence of a mineralizing vasculopathy as the cause, whereas other studies suggest altered perfusion, perhaps the result of impaired autoregulation (33,34). Lenticulostriate vasculopathy is a nonspecific finding, and the diagnosis of congenital infection should not be strongly considered unless other supportive findings (parenchymal regions of hyperechogenicity, intraventricular septations, periventricular necrosis [germinolytic cysts], anterior temporal white matter lesions, and/or abnormalities of sulcation) are also seen by fetal imaging (US or MRI) or postnatal US, CT, or MRI (Fig. 11-4) (35,36,37). Antenatal cranial sonography may offer predictive information for the fetus infected with CMV but may underestimate the presence of anterior temporal lobe or temporal polar abnormalities (38). On CT and MR, some patients, presumably infected during the first half of the second trimester, demonstrate agyria or lissencephaly with a thin cortex, cerebellar hypoplasia, delayed myelination, marked ventriculomegaly, germinal zone cysts, anterior temporal lobe cysts, and periventricular calcification (Figs. 11-3, 11-4, 11-5 and 11-6). Those injured later, presumably in the middle of the second trimester, have more typical polymicrogyria, less ventricular dilatation, and less consistent cerebellar hypoplasia; schizencephaly and infoldings of cortical dysplasia can be seen (Figs. 11-6, 11-7 and 11-8) (39,40). Patients infected near the end of gestation or in the early postnatal period have normal gyral patterns, mild ventricular and sulcal prominence, and damaged periventricular or subcortical white matter with scattered periventricular calcification or hemorrhage (Figs. 11-7, 11-8 and 11-9) (12,18,24,28,41,42). FLAIR images, particularly in the first year of life, provide relatively poor contrast between gray and white matter; therefore, T2-weighted images are essential to identify
cortical malformations (Figs. 11-6 and 11-7), the detection of which helps establish the diagnosis of congenital CMV.
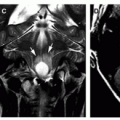
 Figure 11-2 Neurosonographic features of congenital CMV infection. A. Parasagittal sonogram shows linear hyperechogenicity (arrows) within the basal ganglia consistent with lenticulostriate mineralizing vasculopathy. Note the focus of periventricular hyperechogenicity (arrowhead) corresponding to calcification on CT (not shown). B. Coronal sonogram shows multiple subcortical and periventricular foci of hyperechogenicity confirmed by CT (not shown) to represent calcification (arrows). Also note the left germinal matrix cyst (arrowhead). C. Parasagittal sonogram in a microcephalic newborn demonstrates extensive linear and punctuate periventricular hyperechogenicities (arrows) representing calcification. There is moderate ventriculomegaly. D. Parasagittal sonogram shows a cyst of the caudothalamic germinal matrix zone (arrow) and focal peritrigonal hyperechogenicities (arrowheads) consistent with calcification. |
 Figure 11-3 Congenital cytomegalovirus infection. A. Coronal sonogram in this microcephalic newborn shows moderate ventriculomegaly and multifocal periventricular hyperechogenicities (arrows). B. Axial noncontrast CT shows extensive periventricular calcification. Note the moderate ventricular dilatation and overlap of the coronal sutures reflecting underlying brain injury and poor brain growth. C. Axial T1-weighted image at the level of the enlarged lateral ventricles demonstrates ependymal T1 shortening (arrows) representing calcification. D. Axial T2-weighted image shows less conspicuous T2 shortening at sites of known calcification (black arrows). E. Axial T2-weighted image 3 years later shows persistent ventricular enlargement and near-complete absence of periventricular T2 hypointensities. In time, the microglial cells or Hortega cells will remove calcium and hemorrhage. |
 Figure 11-4 Congenital CMV infection. A. Coronal cranial ultrasound shows basal ganglia linear hyperechogenicities consistent with lenticulostriate vasculopathy (arrows). Also note the focal dilation of the temporal horns (arrowheads). B. Axial T2-weighted image demonstrates bilateral cystic temporal horn dilation (curved arrows). Hyperintense white matter is identified anterior to the temporal horns. |
 Figure 11-5 Congenital cytomegalovirus infection in a neonate. A and B. Axial T1-weighted images show the agyria, markedly hypoplastic cerebellar hemispheres (white arrows), and periventricular calcifications (black arrows) common in this disorder. |
detected on CT than on MR in older infants and children. Although dogma has suggested that congenital CMV CNS infection is predictably associated with cerebral calcifications, the prevalence of calcification may be less than 70%. Differentiation of calcification from hemorrhage may be difficult by either CT or MRI (24). Including susceptibility-weighted imaging (SWI) and SWI filtered phase maps into the routine MR examination aids in the differentiation of SWI hypointensities of blood products (paramagnetic) from calcifications
(diamagnetic). The SWI filtered phase map of calcifications is hyperintense (Fig. 11-10) (44). Clinicians should recognize that calcification is not uniquely specific for congenital infection, as any injury to the brain, including those caused by ischemia, genetic syndromes, metabolic errors, and nonspecified neurodegeneration, can cause dystrophic calcification (45,46,47). MR is the imaging examination of choice for the detection of cortical malformations, myelin abnormalities (delay and demyelination), germinal zone cysts, and cerebellar hypoplasia/dysplasia. When these features are present in a child with microcephaly, developmental delay, sensorineural hearing loss, and seizures, a diagnosis of congenital CMV should be considered (24).
 Figure 11-6 Cortical dysgenesis and congenital cytomegalovirus infection. A. Axial noncontrast CT image shows extensive intracranial parenchymal calcification and shallow sylvian fissures strongly suggesting an accompanying neuronal migration anomaly. B. Axial T1-weighted image demonstrates foci of T1 shortening (arrows), which correspond to calcification on CT. Note the simplified perisylvian sulcation. C. Axial T2-weighted image through the posterior fossa shows a hypoplastic cerebellum. Cystic change (arrow) and folial dysgenesis are noted. D. Axial T2-weighted image shows the cortical dysgenesis of the cerebrum to best advantage; this is most likely diffuse polymicrogyria. Note the subtle foci of T2 shortening corresponding to calcification (arrows) and the occipital periventricular cysts. |
 Figure 11-7 Infant with congenital cytomegalovirus infection. A. Sagittal T1-weighted image shows diffuse polymicrogyria (arrows). Also note temporal horn dilation (curved arrow) and T1 prolongation of anterior temporal lobe white matter. B. Axial T2-weighted image at the level of the temporal horns shows bilateral temporal horn dilation and T2 prolongation of temporal lobe white matter. |
 Figure 11-7 (Continued) C. Axial FLAIR image shows simplified sulcal gyral pattern consistent with bihemispheric polymicrogyria (arrows) and confluent regions of cerebral hemispheric white matter T2 prolongation. |
 Figure 11-8 Congenital cytomegalovirus infection with focal clefting and encephalomalacia. A. Axial noncontrast CT image shows bilateral frontal lobe subcortical hypoattenuating regions (black arrows) and sparse parenchymal calcification (white arrow). B. Parasagittal T1-weighted image shows several areas of subcortical encephalomalacia (black arrows), manifested as hypointensity. C. Axial T2-weighted image demonstrates the encephalomalacic regions to be continuous with the subarachnoid space as clefts (white arrows). Also note the other patchy bihemispheric regions of white matter hyperintensity. D. Axial FLAIR image shows to best advantage the confluent regions of bihemispheric white matter hyperintensity and the hypointense subcortical white matter clefts (black arrows). E. DTI-derived axial color-encoded fractional anisotropy (FA) map demonstrates a loss of coherence (hypointensity and distortion of normal tracts, as well as predominant superior-inferior orientation, manifested as blue color) in the periventricular corticospinal tracts (white arrows). |
 Figure 11-9 Congenital cytomegalovirus infection and white matter disease. A. Parasagittal T1-weighted image demonstrates an anterior temporal lobe subcortical cyst (white arrows). Also note confluent T1 prolongation within the parietal white matter (black arrows). B. Coronal T2-weighted image demonstrates anterior temporal cysts (black arrows). Note the multifocal areas of central and subcortical white matter T2 prolongation (white arrowheads). C and D. Axial FLAIR images at the level of the lateral ventricles and centra semiovale show bilateral asymmetric patchy regions of white matter FLAIR hyperintensity. |
of infants with neonatal HSV encephalitis will have negative HSV PCR studies (52). Therefore, a negative result should be interpreted with caution. If there is a clinical suspicion of HSV meningoencephalitis, a second lumbar puncture should be performed and acyclovir administered empirically until the results of the second PCR are known. Therapy of neonatal HSV CNS infections consists of high-dose (60 mg/kg/day) acyclovir for 28 days (54). Infants who survive perinatal HSV infections are at high risk for cerebral palsy, epilepsy, and developmental delay despite aggressive acyclovir therapy (49,52). Suppressive antiviral therapy for 6 months after the initial treatment substantially improves the long-term outcome of neonatal HSV infections (55).
 Figure 11-10 Susceptibility-weighted imaging (SWI) and Ca++ detection. A. Axial NECT in a patient with tuberous sclerosis complex demonstrates focal periventricular highattenuation calcified tubers. B. Axial SWI image shows focal hypointensities where CT demonstrated calcifications. C. Axial filtered phase map of the SWI image demonstrates the calcified tubers as hyperintense foci (arrows). This demonstrates the value of SWI filtered phase maps in discriminating hemorrhage (paramagnetic and SWI-hypointense, filtered phase map hypointense) from calcification (diamagnetic and SWI hypointense, filtered phase map hyperintense). |
elevated lactate and, often, reduction of N-acetyl aspartate (NAA) in affected regions (Fig. 11-12) (61,63). After 1 or 2 days, CT and MR show patchy, multifocal areas of injury (low attenuation on CT, T1 hypointensity, T2 hyperintensity, and regions of reduced diffusion), affecting gray and white matter (Figs. 11-11, 11-12 and 11-13), which progresses in prominence and extent of involvement during the course of the next several days. Hemorrhage is a common finding in neonatal herpes encephalitis, seen in up approximately two-thirds of patients (Fig. 11-14) (63). Contrast enhancement, although minimal, occurs early in a meningeal pattern (Fig. 11-14) (63). Near the end of the first week of disease, there are often regions of cortical gray matter injury (increased attenuation on CT, T1 hyperintensity, and T2 hypointensity on MR) that persists for weeks to months(61,63,67). Loss of brain substance occurs rapidly, often as early as the second week. Eventually, severe, diffuse cerebral atrophy ensues with profound cortical thinning and encephalomalacia; in the end stage, the brain often appears multicystic (Fig. 11-15E). Punctate or curvilinear gyral calcifications may also be seen as a late finding. The cerebellum is injured in about half of the affected patients (61,63,67).
 Figure 11-11 Early diffusion-weighted imaging in neonatal herpes simplex encephalitis. A. Axial noncontrast CT in a seizing 3-week-old female shows diffuse hypodensity. B. Axial T2-weighted image shows normal gray matter and white matter differentiation without cortical blurring. Cortical blurring is an indicator of early peripheral edema. C. Axial apparent diffusion coefficient image shows reduced diffusion within the left temporal lobe (arrows) and occipital poles. Diffusion-weighted imaging is particularly valuable in the early phase of neonatal herpes encephalitis where injury of tissue is manifested as regions of reduced diffusion. |
 Figure 11-12 Multifocal cerebral injury pattern in neonatal herpes encephalitis. A. Parasagittal T1-weighted image shows swelling of the right parietal cortex (arrow). B. Axial T2-weighted image demonstrates T2 prolongation (arrows). C. Coronal FLAIR image shows right thalamic hyperintensity (arrowhead). Also note the focus of right opercular cortical hyperintensity (arrow). D. Axial apparent diffusion coefficient image shows multiple sites of reduced diffusion within the cerebral hemispheres (hypointensities). E. Proton MR spectroscopy (TE = 288 ms) of the thalamus shows diminished NAA peak. Note the elevation of lactate (Lac). Along with diffusion-weighted imaging, magnetic resonance spectroscopy gives insight into early tissue injury. |
(see Chapter 5) and toxoplasmosis. Hydrocephalus, seen in more than 50% of affected neonates, results from necrotizing ependymitis and aqueductal obstruction (70,71). Other infants with congenital LCMV virus infections can have microcephaly and intracranial calcifications (70,71). Seizures commonly develop during the first year of life. Longterm outcome is generally poor, with mortality as high as 35% and severe neurologic sequelae in more than 60% of survivors (71).
 Figure 11-13 Leukotropic neonatal herpes simplex encephalitis. A. Axial T1-weighted image shows bilateral frontal white matter foci of T1 shortening (arrows) likely representing coagulative necrosis of the white matter. There was no corresponding GRE blooming. Also note the focal right germinal zone hemorrhage (arrowhead). B. Axial T2-weighted image demonstrates corresponding T2 shortening (arrows). C. Coronal T2-weighted image shows more hypointense foci within the centrum semiovale of the cerebral hemispheres (arrows). D. Axial diffusion-weighted image shows bifrontal and left peritrigonal foci of hyperintensity (arrows). E. Axial apparent diffusion coefficient image confirms the bright diffusion-weighted signal abnormalities to represent sites of reduced diffusivity (arrows). As the encephalitis becomes less acute, standard spin echo images become more useful and diffusion-weighted imaging less useful. F. Axial color-encoded fractional anisotropy image (F) at the location of previously described reduced diffusion shows disturbance of white matter fiber track coherence: increased anisotropy in corpus callosum but decreased in the frontal and occipital white matter (arrows). |
 Figure 11-14 Hemorrhagic neonatal herpes simplex encephalitis. A. Axial T1-weighted image in a 3-week-old neonate demonstrates right thalamic and left temporal lobe T1 shortening confirmed on GRE imaging to represent hemorrhage. The deep cerebral nuclei and temporal lobes are common sites of injury in neonatal herpes encephalitis. B. Coronal T2-weighted image depicts the multifocality of brain parenchymal involvement that occurs in 67% of neonatal herpes encephalitis. Note the bilateral frontal, right basal ganglia, and left parafalcine parenchymal hemorrhages (T2 shortening) and associated edema (T2 prolongation). C. Coronal GRE shows cortical, subcortical, and basal ganglia regions of blooming hypointensity representing multifocal hemorrhage. D. Axial T1-weighted contrast enhanced image at the level of the lateral ventricles demonstrates bilateral subinsular foci of T1 shortening (arrows). Prior to contrast, no corresponding hyperintense lesions were seen. |
of the world, with more than 100,000 cases estimated by the Centers for Disease Control and Prevention (CDC) to have occurred worldwide annually during the first decade of the current millennium. Humans represent the only reservoir of rubella virus, and transmission results from contact with virus-contaminated respiratory secretions (76).
 Figure 11-15 Progression of neonatal herpes encephalitis to cystic encephalomalacia. A. Axial T1-weighted image in a preterm neonate with new-onset seizures shows a focus of hemorrhage within the right parietal lobe (arrow). There are multiple bilateral centrum semiovale foci of T1 shortening. GRE imaging confirmed hemorrhage in multiple white matter sites. The simplified sulcation and gyration pattern was attributed to prematurity. B. Axial T2-weighted image shows a focal hemorrhage with hematocrit effect in the right parietal white matter. T2 signal is prolonged throughout the white matter. C. Coronal T2-weighted image shows symmetric temporal and frontal white matter T2 hyperintensity. Note the subtle hypointensity within the right temporal white matter (arrow) that corresponded to hemorrhage on GRE. D. Axial apparent diffusion coefficient image at the level of the temporal lobes 14 days after symptom onset shows increased diffusivity throughout the white matter (regions of hyperintensity). E. Axial FLAIR image at 5 years of age shows extensive cystic encephalomalacia. |
 Figure 11-16 Lymphocytic choriomeningitis virus (LCMV). Axial noncontrast CT images (A-C) show a diffuse array of small calcifications involving subcortical and periventricular white matter and internal capsules. This microcephalic infant with chorioretinitis had a “negative” clinical/laboratory evaluation for TORCH infection. The imaging studies of neonates and infants with LCM may be identical to those of neonates and infants afflicted with congenital CMV and toxoplasmosis. |
 Figure 11-17 Lymphocytic choriomeningitis virus. A. Axial noncontrast CT image shows marked hydrocephalus and hypodensity of the white matter, but no calcifications. B. Axial T2-weighted image shows abnormal sulcation (arrows) of the frontal lobes. |
 Figure 11-18 Congenital rubella. A. Axial noncontrast CT demonstrates subtle cerebral calcifications (arrows). B and C. Axial T2-weighted images show patchy regions of periventricular white matter hyperintensity (arrows) most consistent with regions of demyelination and/or gliosis. (Courtesy of Majda M. Thurner, MD, and Elsevier.) |
 Figure 11-19 Congenital syphilis. Axial T2-weighted image shows watershed ischemia in the right cerebral hemisphere and severe ischemic damage in the left cerebral hemisphere. Ischemic injury is due to invasion of perivascular spaces by an inflammatory infiltrate. (Courtesy of Robert A. Zimmerman, MD, Philadelphia, PA.) |
to a more variable outcome; on CT, sparse (Fig. 11-21) or multiple periventricular calcifications and ventricular dilation are typical findings (Fig. 11-20). Infection after the 30th week of gestation is generally associated with mild clinical and imaging abnormalities, with CT findings of small periventricular and intracerebral calcifications that are only rarely accompanied by ventricular dilatation (104). An important differentiating feature between congenital toxoplasmosis and congenital CMV infection is the absence of cortical malformations in toxoplasmosis (a common occurrence in congenital CMV). The brain calcifications of congenital toxoplasmosis may resolve slowly in some infants after antitoxoplasma therapy (106). Therefore, the disappearance of calcification over time should not cause confusion if the diagnosis was established at birth on the basis of characteristic ocular findings and serologic testing.
 Figure 11-20 Congenital toxoplasmosis. A and B. Axial noncontrast CT images in a newborn show extensive parenchymal calcifications that are predominantly cortical and subcortical in location. Also note moderate ventriculomegaly. Hydrocephalus is more common in toxoplasmosis than CMV infection. C and D. Axial and coronal T2-weighted images show multiple foci of T2 hypointensity corresponding to CT confirmed calcification (black arrows). Also note the subcortical cysts (c). Ventriculomegaly is moderate. |
 Figure 11-21 Congenital toxoplasmosis with minimal cerebral calcification. A and B. Noncontrast axial CT images show sparse parenchymal calcification (arrows). Calcification was not present on the initial CT studies in the neonatal period. Note the presence of ventricular shunt catheters. Congenital toxoplasmosis is often associated with ependymitis and resultant hydrocephalus. |
 Figure 11-22 Congenital varicella-zoster virus infection. A. Axial T1-weighted image in a microcephalic term newborn shows extensive bilateral periventricular T1 shortening consistent with coagulative necrosis. SWI showed no evidence of hemorrhage or calcification. B. Axial T2-weighted image shows no significant abnormality. Note the normal cortical ribbon at this level, unlike polymicrogyria often observed in congenital CMV infection. C. Axial ADC map demonstrates scattered foci of reduced diffusion (arrows). |
 Figure 11-23 Congenital Zika virus infection. Axial noncontrast CT in a microcephalic newborn shows bilateral cerebral hemispheric calcifications predominantly at the gray matter/white matter junctions. Also note the simplified sulcal gyral pattern and widened lateral cerebral fissures consistent with extensive bilateral polymicrogyria (arrows). Overlapping of the cranial sutures reflects micrencephaly. (Courtesy of Andres Pessoa, MD, Fortaleza, Brazil.) |
 Figure 11-24 Congenital Zika virus infection. A. Sagittal T1-weighted image demonstrates decreased cranial-to-facial ratio consistent with microcephaly. Also note the frontal lobe region of T1 shortening consistent with calcification at the gray matter/white matter junction (arrow). B. Axial T1-weighted image confirms regions of T1 shortening consistent with calcifications (arrows). C. Axial T2-weighted MR image shows diffuse bilateral cerebral hemispheric simplified sulcal gyral pattern consistent with polymicrogyria (arrows). (Courtesy of Lara Brandao, MD, Rio de Janeiro, Brazil.) |
opportunistic infections with T. gondii, cytomegalovirus, varicellazoster virus (VZV), Mycobacterium tuberculosis, fungi, and JC virus, the cause of progressive multifocal leukoencephalopathy (PML) (131).
 Figure 11-25 Neonatal parechovirus encephalitis. A. Axial T2-weighted image at the level of the centrum semiovale shows patchy regions of T2 shortening and prolongation (arrows). B. Axial diffusion-weighted image demonstrates confluent areas of subcortical and central white matter signal hyperintensity. C. Axial apparent diffusion coefficient image at the level of the frontal horns shows cortical and subcortical white matter regions of bihemispheric hypointensity (white arrows), including the left caudate head (black arrow), indicating reduced diffusivity. (These images courtesy of Linda S. de Vries, MD, PhD, Utrecht, Netherlands.) |
associated encephalopathy; therefore, imaging studies of the spine in children with HIV myelopathy are uncommon.
 Figure 11-26 Encephalitis secondary to congenital AIDS. A. Axial noncontrast CT image at age 1 year shows mild prominence of the ventricles and subarachnoid spaces with mildly increased attenuation in the basal ganglia (arrows). B. Follow-up axial noncontrast CT image at age 2 years shows marked calcification of the lentiform nuclei (straight arrows) and subcortical frontal white matter (curved arrows). |
 Figure 11-27 Aneurysmal arteriopathy in an HIV-infected child. A. Axial time-of-flight (TOF) MRA source image at the level of the anterior clinoids shows enlarged supraclinoid carotid arteries (arrows). B. Axial TOF MRA image at the level of the pentagonal cistern shows fusiform aneurysms of the middle cerebral artery M1 segments (arrows). |
 Figure 11-28 Genetic syndrome that mimics congenital infection. Aicardi-Goutieres syndrome. A. Axial CT through the posterior fossa shows pontine calcifications (arrows). B. Axial CT at the level of the third ventricle demonstrates bilateral thalamic calcifications centrally and numerous peripheral calcifications. C. Axial CT at the level of the lateral ventricles shows extensive periventricular calcification. Also note the passive ventricular dilation secondary to periventricular white matter volume loss. The brain stem and basal ganglia calcifications are not common in TORCH infections. |
Unlike previously discussed infections such as CMV, which reflect a static pattern of brain injury and/or malformation, the infant and young child with ACS exhibit progressive neurodegenerative clinical and neuroimaging findings.
 Figure 11-29 Genetic syndrome that mimics congenital infection. Adams-Oliver syndrome. Axial noncontrast CT image demonstrates extensive periventricular calcification and ventriculomegaly in this microcephalic infant. |
 Bacterial, Spirochetal, and Rickettsial Infections
Bacterial, Spirochetal, and Rickettsial Infectionsof all ages in the United States and other regions with widespread use of the Hib vaccine and newer vaccines for both S. pneumoniae and N. meningitidis (167). Nontypeable Haemophilus influenzae or non-b subtypes have emerged as clinically important agents causing meningitis among healthy or immunocompromised children in many regions, including those with compulsory immunization against H. influenzae (Table 11-4) (4,174,175,176). Subtypes of H. influenzae remain important causes of bacterial meningitis with subtype F representing an aggressive, regional, circum-polar infection with reports often originating in remote northern latitudes. Subtype A and nontypeable H. influenzae are often associated with milder cases of meningitis. Among unimmunized children, H. influenzae meningitis occurs more commonly in persons with sickle cell anemia, asplenia, and HIV infection, and generally in older infants. Other risk factors for S. pneumoniae meningitis also include nephrotic syndrome, cochlear implantation, and CSF leaks. Unimmunized college students and persons with inherited complement deficiencies have an increased risk of contracting N. meningitides meningitis. Children or adolescents with congenital or acquired immunodeficiencies, including disorders of cell-mediated immunity or granulocyte function, can experience meningitis due to Pseudomonas aeruginosa, Staphylococcus epidermidis, Staphylococcus aureus, Listeria monocytogenes, and enteric organisms (174). Meningitis also represents one of the most common extrapulmonary manifestations of infection with Mycobacterium tuberculosis (177).
Table 11-3 Selected Causes and Imaging Features of Neonatal Bacterial Meningitis | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Table 11-4 Common Causes of Bacterial Meningitis in Infants, Children, and Adolescents | ||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||||||
 Figure 11-30 Uncomplicated neonatal Group B Streptococcus (S. agalactiae) meningitis. A. Coronal cranial sonogram shows echogenic widening of the sulci (arrows). Also note the expansion of the subarachnoid spaces. B. Sagittal cranial sonogram also shows echogenic widening of the sulci (arrow). Normally, the pia-arachnoid membrane should not exceed 2 mm in thickness. This thickened sulcus measured 4 mm. Note the expanded subarachnoid space. Color Doppler ultrasound (not shown) is useful in assigning the location of the extra-axial fluid (subdural vs. subarachnoid). C. Postcontrast coronal T2 FLAIR image shows extensive leptomeningeal enhancement. This is particularly well seen within the lateral cerebral fissures (arrows). Note the expanded convexity subarachnoid spaces. No complications of meningitis were encountered. |
controls, neonates with meningitis have increased FA values in the LCSWM, likely reflecting the presence of inflammatory adhesion molecules within the subarachnoid space (192).
 Figure 11-31 Bacterial meningitis and effusions (subarachnoid and subdural). A. Axial noncontrast CT image of a 4-year-old male with Non-type b encapsulated Haemophilus Influenzae meningitis. Symmetric frontal extra-axial fluid collections similar to CSF in attenuation (arrows). Subdural effusions were favored. B. Axial T1-weighted image shows frontotemporal fluid collections isointense to ventricular CSF. A membrane with increased signal intensity traverses the left frontal subarachnoid space (arrow). C. Axial T2-weighted image shows numerous veins coursing through the expanded subarachnoid spaces (arrowheads). This supports that the effusion is primarily subarachnoid in location. A thick hypointense membrane is seen in the left subarachnoid space (arrow). D. Axial FLAIR image shows to better advantage several membranes within the left frontotemporal extra-axial space (arrows). |
 Figure 11-31 (Continued) E. Axial diffusion-weighted image shows subtle signal increase at the site of previously described membranes (arrows), but the effusions show no evidence of diffusion restriction. F. Postcontrast coronal T1-weighted image shows numerous enhancing veins coursing through the supratentorial subarachnoid spaces (subarachnoid effusions). Note the medial displacement of the left frontal veins (arrows) by a mildly compressive subdural effusion. |
 Figure 11-32 Subdural effusions and empyema in type F Haemophilus influenzae meningitis. A. Coronal T2-weighted image shows compressive bilateral frontal subdural fluid collections. Note the hypointense cortical veins adjacent to the brain surface (arrows). B. Axial FLAIR image through the cerebral convexities shows increased FLAIR signal within the right frontal subdural collection. Signal within the left subdural collection approximates CSF. Note the increased signal within the sulci reflecting leptomeningeal inflammation (arrowheads). The patient was not sedated under general anesthesia or with the use of fentanyl, both of which can produce increased FLAIR signal within the subarachnoid space. C. Axial average diffusivity image (ADC) through the convexities shows regions of hypointensity within the right subdural collection indicating reduced diffusion (empyema) (arrows). Note the component of the right subdural collection that shows increased diffusivity (more rapid water movement, arrowheads). D. Coronal postcontrast T1-weighted image shows mass effect of the convexity subdural collections. Note the thick right endosteal dural (arrowheads), and meningeal dural and leptomeningeal (arrows) enhancement. Due to seizures and persistent fever, the patient required right frontal subdural drainage. |
 Figure 11-33 Subdural empyema complicating Streptoccocus pneumoniae meningitis. A. Axial noncontrast CT image shows a diminished attenuation left parafalcine subdural fluid collection (white arrows). B. Axial T2-weighted image performed within 24 hours of the CT shows bilateral hyperintense parafalcine collections (white arrows). C. Axial apparent diffusion coefficient (ADC) image shows hypointense signal (white arrows) within the subdural fluid confirming reduced diffusion secondary to viscous purulent material. D. Axial postcontrast T1-weighted image shows marginal enhancement of the dural borders and prominent leptomeningeal enhancement secondary to meningitis. Postcontrast MR imaging is very useful in detecting small empyemas of the convexities, within the middle cranial fossa, and adjacent to the tentorium. |
is uncertain, or a complication of meningitis is suspected (Fig. 11-37). Hydrocephalus complicating meningitis indicates altered CSF circulation and/or resorption, which may occur at several levels (Fig. 11-38) (4,6,194), reflecting the intense inflammatory reaction and purulent exudates within the interventricular communications pathways, basal cisterns, sulci, and perivascular spaces (Figs. 11-37 and 11-38).
 Figure 11-34 Subdural empyema, a complication of sinusitis. A and B. Axial T1 (A) and T2 (B) weighted images show a left parafalcine and left frontal subdural empyema (arrows). C. Axial diffusion-weighted image demonstrates hyperintensity (arrows) of the empyema secondary to the viscous nature of the purulent material. D. Coronal postcontrast T1-weighted image shows the empyema fluid (e) to be slightly hyperintense to CSF. There is underlying meningeal enhancement and outer dural enhancement. Note the moderate mass effect and left to right subfalcial herniation. Intracranial empyemas may evolve remote from the infected paranasal sinus. Thus, whole brain imaging is warranted when evaluating for suspected complications of sinusitis. E. Axial postcontrast FLAIR image clearly demonstrates the meningeal (inner) and endosteal (outer) margins of subdural compartment empyema enhancement. |
 Figure 11-35 Ventriculitis secondary to Escherichia coli. A and B. Coronal (A) and parasagittal (B) cranial sonograms show septated material filling and expanding the lateral ventricles (arrows). Note the hyperechoic thickening of the frontal horn ependyma (ependymitis, arrowheads in B). C. Axial T2-weighted image shows dependent debris (d) within the atria of the lateral ventricles. There is evidence for early ventricular obstruction. D. Axial diffusivity image shows hypointense signal within the occipital horns (arrows) and the right sylvian cistern subarachnoid space (arrowheads) consistent with reduced diffusion from highly viscous purulent material. E. Axial postcontrast T1-weighted image demonstrates dependent ventricular debris (d) and the thickened enhancing ependyma (white arrowheads) in ventricular trigones and occipital horns. Also note the prominent leptomeningeal enhancement within the sylvian cisterns. |
 Figure 11-36 White matter necrosis secondary to ventriculitis. A. Axial T1-weighted image shows proteinaceous debris (white arrowheads) layering in the posterior portion of the lateral ventricles. Early white matter necrosis is seen as mixed areas of hyper and hypointensity (small white arrows) in the frontal lobes. Poor gray matter-white matter contrast is seen in the entire cerebrum. B. Axial T2-weighted image shows extensive white matter necrosis (white arrows) seen as hypointensity of the white matter with some surrounding hyperintense edema. C. Postcontrast T1-weighted image shows better, the extent (small white arrows) of frontal necrosis. Some of the necrosing tissue (white arrowheads) is enhancing. The walls of the lateral ventricles (black arrowheads) are enhancing posteriorly. D. Follow-up postcontrast T1-weighted image 6 weeks later shows hydrocephalus and cavitation of the frontal lobes. Note that proteinaceous debris (white arrowheads) layering dependently within the ventricles. Some loculations (L) have formed adjacent to the ventricles. |
partition size (158) (see discussion on the following page). This observation is most easily made on midline sagittal images encompassing the sagittal sinuses and straight sinus/vein of Galen complex and on parasagittal images for the transverse and sigmoid sinuses. Other than in the subacute phase, the MR diagnosis of sinus thrombosis is difficult. Pronounced hypointensity seen in a venous sinus on sagittal T1-weighted images or in the superior sagittal sinus on coronal FLAIR images mitigates against thrombosis. However, in the absence of pronounced hypointensity on T1-weighted images, the patency of the sinus remains uncertain on routine MR images (Figs. 11-39B and 11-40A). The acutely thrombosed sinus is isointense to the brain on T1-weighted images and hypointense to the brain on T2-weighted images. This appearance cannot be distinguished from slow flow or pseudogating (in which the sinus is imaged during diastole). In this situation, evaluating the SWI images and reformations is very helpful to look for the hypointensity (paramagnetic effect) of thrombosis. Overall, as mentioned above, intravenous contrast-enhanced 3D MRV techniques are superior in the detection of cerebral sinovenous thrombosis as well as cortical and bridging vein thromboses (Figs. 11-40E and 11-41B) (158). In the clinical setting where contrast is contraindicated, robust noncontrast time-of-flight (TOF) 3D MRV contributes useful information.
 Figure 11-37 Early hydrocephalus secondary to non-type b Haemophilus influenzae meningitis. A and B. Axial noncontrast CT images demonstrate infectious debris adjacent to the falx cerebelli (arrows) and dilation of the temporal horns (arrowheads) and third ventricle. The cerebrum is low in attenuation and there is absence of gray matter-white matter contrast. C. Coronal postcontrast T1-weighted image from MR 48 hours following the CT shows progressive dilation of the lateral and third ventricles. D. Axial postcontrast FLAIR image at the level of the basal cisterns demonstrates diffuse enhancement of the basal cisterns (white arrows). CSF flow is obstructed at this level. |
 Figure 11-38 Hydrocephalus following Escherichia coli meningitis. A. Four weeks following the completion of therapy for E. coli meningitis, Axial T2-weighted image in this infant with a bulging anterior fontanelle shows focal encephalomalacia of the brain stem secondary to remote brain stem infarction (arrow). There is moderate dilation of the temporal horns. B. Axial T2-weighted image at the level of the third ventricle demonstrates moderate dilation of the lateral ventricles and third ventricle. There is stretching of the massa intermedia (black arrowhead). Also note the lack of normal hypointense signal within the cerebral aqueduct (black arrow), indicating disturbance of normal CSF flow. This represents postmeningitic noncommunicating hydrocephalus. |
 Figure 11-39 Sagittal sinus thrombosis secondary to meningitis. A. Noncontrast CT scan shows high attenuation in the torcular herophili (arrows) at the junction of the straight sinus (also hyperdense and thrombosed) and the superior sagittal sinus. The presence of high density within blood vessels in a child beyond the first few months of life is extremely suspicious for sinus thrombosis. B. Sagittal T1-weighted image shows high signal intensity in the posterior half of the superior sagittal sinus (black arrows). The straight sinus (white arrowheads) also appears thrombosed. C. Coronal FLAIR image shows high signal intensity (arrow) within the superior sagittal sinus, supporting the diagnosis of sagittal sinus thrombosis. D. Axial T2-weighted image shows hyperintensity in the sagittal sinus (white arrows), suggesting the presence of extracellular deoxyhemoglobin, present in subacute clot. E. 2D time-of-flight MR venogram shows absence of flow-related enhancement in the superior sagittal sinus, confirming the diagnosis of thrombosis. |
 Figure 11-40 Streptococcus pneumoniae meningitis, venous thrombosis and cerebral ischemia. A. Axial T2-weighted image shows right cerebral convexity regions of subcortical T2 prolongation (edema) (arrows). B. ADC map shows reduced diffusion involving the right frontoparietal convexity (arrow). C. Axial SWI shows numerous right convexal serpentine hypointensities consistent with slow flow or thrombus within convexity veins (arrows). D. Axial T1-weighted following intravenous contrast shows filling defects (clot) within the right convexity veins (arrows). E. Sagittal post-IV contrast 3D SPGR image demonstrates clot within the right transverse venous sinus (arrow). |
 Figure 11-41 Cortical vein thrombosis and cerebral ischemia secondary to Neisseria meningitides meningitis. A. Coronal GRE image shows several convexity cortical veins demonstrating diminished signal indicating cortical vein thrombosis or slow venous flow. B. Axial postcontrast T1-weighted image shows thick enhancement within the left intraparietal sulcus (large white arrows). Note the linear hypointense filling defect (small black arrow) consistent with thrombosed cortical vein. The adjacent cortex shows T1 hypointensity consistent with edema. Also note the bilateral frontal effusions. C. Axial average diffusivity image shows evidence of increased diffusivity (interstitial edema, white arrows). There is reduced diffusivity (hypointensity, white arrowheads) adjacent to the lateral intraparietal sulcus, suggesting injured tissue. Cortical venous occlusion leads to regional venous hypertension, breakdown of the blood-brain barrier and, sometimes, ischemic injury. D. DTI-derived color fractional anisotropy image through the cerebral convexities shows a loss of coherence (decreased anisotropy, arrows) of water motion in the region of the cortical occlusion and in the subcortical white matter tracts, reflecting interstitial edema and, possibly, microstructural white matter injury. |
from sagittal sinus thrombosis are parasagittal (Fig. 11-40); infarcts from thrombosed internal cerebral veins, straight sinus, and vein of Galen involve the thalami. Infarcts from vein of Labbé, transverse sinus, or sigmoid sinus thrombosis involve the temporal lobe. Smaller cortical/subcortical infarcts are often seen over the cerebral convexities (Fig. 11-41). On CT, venous infarcts are usually poorly delimited, hypoattenuating, or mixed attenuation areas involving the subcortical white matter and producing a slight mass effect on ventricular structures. The low attenuation is probably due to localized cerebral edema (vasogenic and cytotoxic), whereas high attenuation areas within the brain parenchyma usually represent hemorrhage. Following intravenous contrast administration, a lack of expected venous opacification is seen (venous clot may be detected), adjacent sulcal/gyral enhancement is noted, and adjacent parenchymal hypoattenuation (edema) is appreciated (209). On MR, early venous infarcts may be identified by visualization of prolonged T1 and T2 relaxation times in characteristic regions of the brain parenchyma, SWI hypointensity within the adjacent venous structure(s), and low ADC values in regional parenchyma (Fig. 11-41). Another early and important imaging sign of venous infarction is visualization of thrombus in the deep medullary veins with surrounding cavitation. Of note, reduced parenchymal diffusivity in the setting of venous thrombosis lacks sensitivity in predicting venous infarction. With venous ischemia and infarcts, diffusion appears to be heterogeneous, with areas of increased, normal, and decreased diffusion (Fig. 11-41) (210). The variable diffusion characteristics are likely related to the combination of interstitial and cytotoxic edema found in venous infarcts. In addition, part of this heterogeneity may be due to the frequent presence of hemorrhagic tissue, which makes diffusivity values unreliable. Twenty-five percent of venous infarcts are hemorrhagic and have an imaging appearance that varies from large subcortical hematomas to petechial hemorrhages admixed with edematous brain parenchyma (Fig. 11-40) (207,209). The hemorrhages are generally subcortical and often multifocal with irregular margins. They are occasionally linear in nature, indicating hematoma in and around the vein; this appearance is quite specific.
or predominant lymphocytic pleocytosis, elevated protein (usually between 100 and 500 mg/dL), and mildly reduced glucose (234). The diagnosis of tuberculous meningitis can be established by PCR detection of mycobacteria in the CSF and supported by a positive tuberculin skin test or detection of interferon-gamma release in whole blood samples exposed to M. tuberculosis antigens (232,234). Treatment consists of combined antituberculous therapy with a four-drug regimen and administration of corticosteroids; even with therapy, death or significant morbidity is possible, especially when treatment is delayed.
 Figure 11-42 Cavernous sinus thrombosis in the setting of sphenoid sinusitis/meningitis. A. Axial contrast-enhanced CT shows enlarged tubular serpentine thrombosed superior ophthalmic veins (white arrows). Note the thrombus within the cavernous sinuses (arrowheads) and the extensive preseptal and postseptal edema. B. Axial T2-weighted fat-saturated image confirms enlarged tortuous thrombosed superior ophthalmic veins (arrows). C. Axial postcontrast axial fat-saturated T1-weighted image shows the thrombosed orbital venous structures as nonenhancing elements. Enhancement is due to multiple small collateral veins. Note the diffuse pre- and postseptal edema. D. Axial postcontrast T1-weighted image through the cavernous sinus demonstrates thrombus as large hypointense filling defects (black arrows). |
causing infarction of surrounding brain tissue. Outcome is directly related to the location and extent of these infarctions (238). The basal ganglia and thalami are affected in almost half of cases (239,240); suprasellar cisternal inflammation and involvement of the posterior hypophysis may lead to the syndrome of inappropriate antidiuretic hormone secretion (241). The thick exudate blocks the subarachnoid spaces, causing hydrocephalus. Infiltration of the perineurium of the cranial nerves causes neuropathies, particularly of cranial nerves II, VI, and VII. Small tubercles over the convexity of the brain may involve the leptomeninges, while deeper lesions may infiltrate the periventricular area.
 Figure 11-43 Multiple perforator arterial infarctions from Group B Streptococcus (S. agalactiae) meningitis. A. Axial T2-weighted image shows innumerable basal ganglia foci of T2 prolongation. Note the subinsular regions of T2 hyperintensity and heterogeneous left perifrontal white matter signal (coagulation necrosis of white matter, black arrow). B. Axial T2-weighted image at the level of the centrum semiovale demonstrates heterogeneous white matter signal intensity (arrows). C and D. Average diffusivity images corresponding to (A and B) show markedly reduced diffusivity corresponding to tissue injury. Note the confluent reduced diffusivity within the centrum semiovale. E. Proton spectroscopy (TE = 35 ms) of the right basal ganglia demonstrates a large lactate/lipid (L/L) and lipid (Li) peaks. Lactate is an indicator of anaerobic metabolism and lipid results from cell necrosis. There is mild decline of NAA and elevation of the excitatory neurotransmitter glutamate and glutamine (Glx). |
 Figure 11-44 Multiple arterial infarctions from Streptococcus pneumoniae meningitis. A. Axial noncontrast CT shows multiple wedge-shaped cortical and subcortical regions of diminished attenuation (white arrows). Numerous basal ganglia/thalami foci of low attenuation are also seen (arrowheads). B. Axial T2-weighted image shows better the regions of peripheral and central T2 hyperintensity representing edema (cytotoxic and vasogenic in type). C. Axial diffusion-weighted image shows multiple sites of ischemic injury as areas of hyperintensity. D. Axial average diffusivity image 6 days after initial diagnosis demonstrates evidence of early pseudonormalization. Relatively few areas of subtle frontal and occipital reduced diffusivity (white arrows) and central basal ganglia and periventricular foci of reduced diffusion (arrowheads) are still seen. |
Related posts:




Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


