Overview
Location
• The inferior vena cava (IVC) originates at the junction of the two common iliac veins anterior to the body of the fifth lumbar vertebra. The IVC is vertically oriented in the body; it ascends through the retroperitoneum (portion of abdominopelvic cavity posterior to the peritoneal sac) anterior and just to the right of the spine and then passes through the diaphragm to enter the right atrium of the heart.
• As the IVC ascends through the retroperitoneum on its way to the heart it passes through a deep fossa on the posterior surface of the liver between the caudate lobe and bare area.
Anatomy
• The inferior portion of the body’s largest vein.
• Consists of 3 muscle layers:
1. Intima (innermost)
2. Media (middle layer)
3. Adventitia (outer)
• Tributaries:
1. 3 hepatic veins
2. 2 renal veins
3. 2 common iliac veins
4. Right adrenal vein
5. Right ovarian vein or testicular vein
6. Inferior phrenic vein
7. 4 lumbar veins
8. Medial sacral vein
• Size is variable and normal up to 4 cm
• Can be very tortuous (marked by twists, turns, or bends)
Physiology
• The IVC returns deoxygenated blood from the tissues to the heart for oxygenation and recirculation.
Sonographic Appearance
• Anechoic lumen surrounded by bright, echogenic walls.
• During real-time examination it is not uncommon to visualize multiple, small, moving echoes within the lumen of the IVC, which are thought to be related to the flow of blood.
• During real-time evaluation the IVC demonstrates significant variation in diameter relative to arterial vessels. The IVC is seen to increase in size with deep inspiration or the Valsalva maneuver (exhaling with airways closed–mouth shut, nose pinched shut) and decrease in size during expiration. Note that a momentary collapse of the IVC can be observed by having a patient “sniff.”
• Since the IVC is vertically orientated in the body, longitudinal and long axis views are seen in coronal scanning planes and sagittal scanning planes as demonstrated in the following image. The IVC appears like a large long tube, anechoic with thin, bright walls, immediately anterior to the spine and right renal artery and immediately posterior to the head of the pancreas, portion of the distal common bile duct, portion of the portal vein, and the right lobe of the liver. Note that the space between the IVC and the spine affords passage of the right renal artery, seen here in an axial section, on its way to the right kidney.

• Short axis (or axial) sections of the IVC are seen in transverse scanning planes. The following transverse scanning plane image shows how easy it is to recognize the short axis section of the mid portion of the IVC in the posterior portion of the image, immediately anterior to the right renal artery and anterior and just to the right of the spine, and immediately posterior to the head of the pancreas and the gallbladder. It appears large, round, anechoic with bright, thin walls, and at this level the right and left renal vein tributaries are easily identified. Notice how the space between the IVC and the spine affords passage of the right renal artery, seen here in a longitudinal section, on its way to the right kidney.

• The proximal (closest to origin) portion of the IVC is described as the area seen extending from its origin at the common iliac veins to the area just inferior to the renal vein tributaries.
• The mid portion of the IVC is seen at the level of the renal vein tributaries, posterior to the head of the pancreas.
• The distal (farthest from origin) portion of the IVC is seen extending from the area just superior to the renal vein tributaries to the right atrium of the heart; it includes the hepatic vein tributaries located just inferior to the diaphragm.
• The 3 hepatic veins, 2 renal veins, and 2 common iliac veins are the IVC tributaries that are routinely visualized with ultrasound. The remaining tributaries are usually too small to distinguish.
Normal Variants
• Duplication.
• Total or partial absence.
• May be particularly short.
• Visceral transposition lying to the left of the aorta.
• Crosses to lie to the left of the aorta.
• Joins with the azygos vein; enters the superior vena cava.
Preparation
Patient Prep
• The patient should fast for at least 6 to 8 hours before the ultrasound examination.
• If the patient has eaten, still attempt the examination.
Transducer
• 3.0 MHz or 3.5 MHz.
• 5.0 MHz for thin patients.
Breathing Technique
• Normal respiration or deep, held respiration.
Patient Position
• Supine.
• Left lateral decubitus, right lateral decubitus, left posterior oblique, right posterior oblique, or sitting semierect to erect as needed.
Inferior Vena Cava Survey Steps
Inferior Vena Cava • Longitudinal Survey
Sagittal Plane • Transabdominal Anterior Approach
1. Begin scanning with the transducer perpendicular, at the midline of the body, just inferior to the xiphoid process of the sternum.

2. Slightly move or angle the transducer to the patient’s left and identify the longitudinal, anechoic, section of the proximal aorta just posterior to the liver.

3. Return to the midline and slightly move or angle the transducer to the patient’s right; identify the longitudinal, anechoic, section of the distal IVC just posterior to the liver.

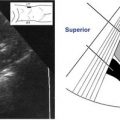
4. While viewing the distal IVC, it may be necessary to slightly twist/rotate the transducer, first one way, then the other, to resolve the longest sections and long axis of the IVC. When the long axis is located, barely twisting/rotating the transducer can help resolve the hepatic vein tributaries, which are seen within the liver, emptying into the IVC anteriorly (Figure 5-1, A). Now, very slightly rock or move the transducer from right to left, scanning completely through each side of the IVC. Continue this and slowly slide the transducer inferiorly following along the length of the IVC. Keep your eyes on the screen; use the image as a guide, evaluating the appearance of the mid and proximal IVC until you reach the right and left common iliac veins (usually at or just beyond the level of the umbilicus).

Related posts:



Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


