31 Infraclavicular Block
Infraclavicular block of the brachial plexus was developed as a means to achieve complete brachial plexus anesthesia and was one of the first blocks to be described using ultrasound imaging.1,2 This block is performed at the level of the pectoralis minor muscle. In this location the brachial plexus consists of three cords that compactly hug the walls of the second part of the axillary artery.3 The infraclavicular region has the advantage of being a secure place for a catheter that provides complete brachial plexus anesthesia. Another advantage is that anatomic variation is relatively uncommon in this region. In the infraclavicular region, the serratus anterior and subscapularis muscles form the margin of safety between the neurovascular bundle and the chest. Because proximal arm muscles are anesthetized (including the pectoralis and deltoid), infraclavicular blocks produce excellent tourniquet tolerance and conditions for upper extremity surgery.4 The block can be performed with the arm abducted or at the patient’s side (Table 31-1).
Table 31-1 Clinical Considerations for Infraclavicular Block
| Advantages | Disadvantages |
|---|---|
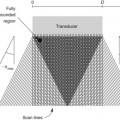
Cord topography changes along the length of the axillary artery in the infraclavicular region.5 Proximally, the cords of the brachial plexus have more of a “supraclavicular” configuration in which all the cords are on the lateral side of the axillary artery. Following distally, the true “infraclavicular” configuration is when all cords surround the axillary artery before the takeoff of the axillary and musculocutaneous nerves. When the transducer is too proximal, the curved inclination of the ribs and pleura can be recognized. When the transducer is too distal, the coracobrachialis muscle and musculocutaneous nerve can be appreciated on the lateral side of artery.