making sure that the connection is tight so that air bubbles are not drawn into the syringe. Contrast material is run through the tubing until all air bubbles are removed from the system. Topical anesthesia and dilators are not needed for this procedure.
Table 11.1: Common Assumptions in Women with Nipple Discharge | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||
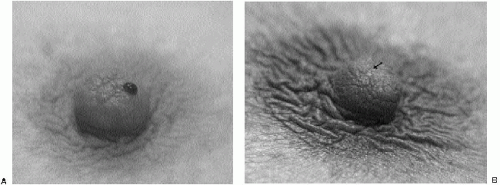 Figure 11.1 Spontaneous nipple discharge. A. Spontaneous bloody nipple discharge arising from a single duct opening. B. Spontaneous clear nipple discharge (arrow) arising from a single duct opening. If the patient presents with spontaneous nipple discharge, the character of the discharge does not dissuade us from evaluating the patient with ductography. Breast cancers can present with clear, or serous, heme occult-negative discharge. |
 Figure 11.2 Duct cannulation. After the duct producing the discharge is identified, the cannula is angled, and the tip is placed in the duct opening. Next, the cannula is gently straightened. In most patients, the cannula falls in the duct to the hub. No pressure is exerted. The patient should experience no pain during cannulation. |
Occasionally, a contained contrast blush is seen, the overall appearance of which suggests the possibility of lobular opacification (Figure 11.8). We use the sialography cannula as an internal measure of duct caliber. Arbitrarily, we define normal duct caliber as up to 3 times the width of the cannula.
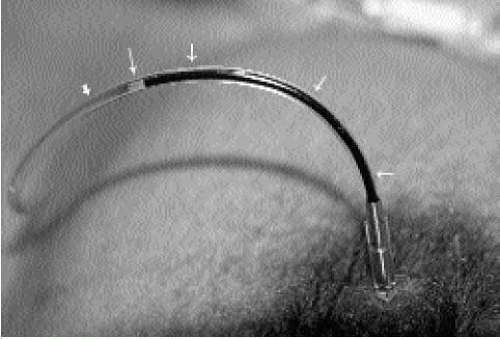 Figure 11.3 Reflux of duct contents into tubing. Cannula in the duct to the hub. Immediately after cannulation, observe the tubing for a few seconds before injecting contrast. The tubing is now in a closed system with the cannulated duct such that duct contents can sometimes be seen refluxing into the tubing. If this is seen, it confirms cannulation of the duct producing the discharge. In this patient, the refluxing material is bloody (short, thin arrows). An air bubble (long, thin arrow) separates the refluxing duct contents from the contrast (thick arrow). When the discharge is clear or serous, mixing of the duct contents with the contrast can be seen occurring in the tubing. |
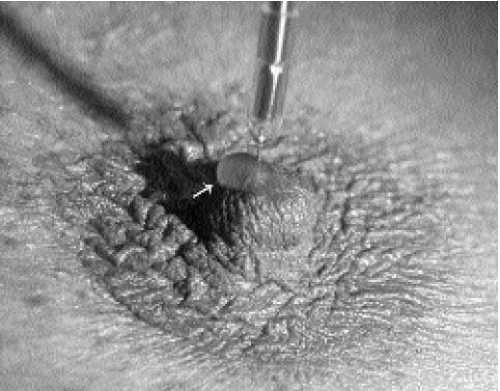 Figure 11.4 Duct contents forming droplet around cannula. If duct contents do not reflux into the tubing, duct contents can sometimes be seen forming a droplet (arrow) around the cannula as contrast is injected. The contrast displaces duct contents. When this is seen, it confirms cannulation of the duct producing the discharge. |
duct ectasia as the cause of nipple discharge (7). These ducts are dilated in the subareolar region and often change abruptly in caliber as the duct courses proximally (Figure 11.15).
 Figure 11.5 Taping cannula in place. After 0.2 to 0.4 mL of contrast is injected, the cannula is taped onto the nipple using two pieces of paper tape. Leaving the cannula in place permits additional injections of contrast as needed to evaluate the duct. The cannula also helps minimize the amount of contrast that is forced out of the duct when compression is applied. |
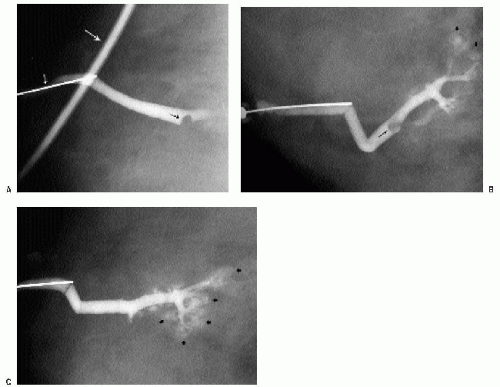 Figure 11.6 Masking of lesion; lobular blushing; papilloma. A. Initial films following injection of 0.2 mL of contrast demonstrate a filling defect (arrow) in a mildly dilated duct. No proximal opacification is noted. Cannula (short thin arrow) is present; tubing with contrast (long thin arrow) should be moved out of the field of view by the technologist. B. After an additional 0.2 mL of contrast, the filling defect (thin arrow) is still seen. Branches of the duct are now filling with contrast, and there is some “blushing” (thick arrows), possibly reflecting contrast in the lobular units. C. An additional 0.2 mL of contrast is injected. The lesion is no longer seen because of the amount of contrast injected. Increased amount of blushing is noted (thick arrows). Small lesions and lesions that are close to the nipple can be obscured if too much contrast is injected initially. A small amount is injected initially. If the cannula is left in place, it is easy to inject additional contrast as needed to evaluate the duct proximally. |
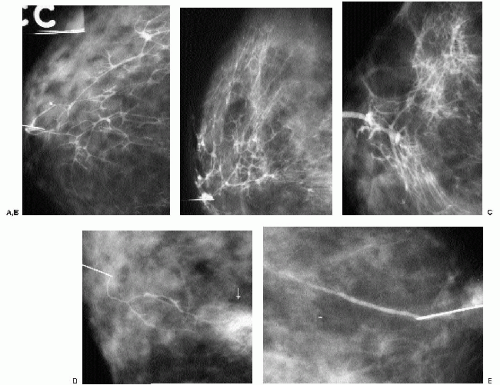 Figure 11.7 Normal ducts. A. Using the cannula as an internal measure, this duct is normal in caliber. This duct demonstrates a wide area of drainage with a moderate amount of branching. No focal abnormality is apparent. B. Different patient. Normal caliber duct (cannula at nipple) with a wide area of drainage and more branching than seen in the previous patient. C. Different patient. The subareolar portion of the duct is at the upper limits for what we define as a normal caliber. Significant branching and a wide distribution in the parenchyma. D. Different patient. In contrast to the prior examples, this duct is attenuated with a minimal number of branches and a limited drainage area. In these smaller ducts, proximal extravasation of contrast (arrow) is seen as attempts are made to distend the duct further. E. Different patient. This duct has no detectable branch points, and its distribution is limited in the breast. Normal caliber. |
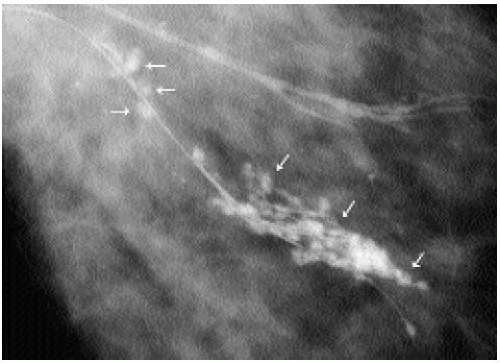 Figure 11.8 Lobular blush; normal duct. In some patients, a contained contrast blush is seen in a lobular-like distribution (arrows) around the duct. This is often seen in normal-caliber ducts such as those seen in this patient. Scattered benign calcifications are seen in the surrounding tissue. |
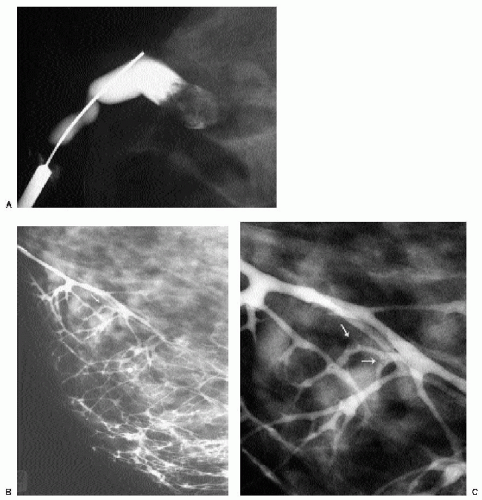 Figure 11.9 Papillomas. A. A lesion is present obstructing the cannulated duct close to the nipple. The irregular interface at the obstructing site reflects contrast pooling in the interstices of the papilloma. The duct between the lesion and the nipple is dilated (compare to cannula). The subareolar location of this lesion, within a distended duct, is a common presentation for papillomas. B. Different patient. The lesion (arrow) is obstructing one of the terminal branches in this duct. The duct is normal in caliber, and there is a significant amount of branching and a wide area of drainage. Despite the magnification technique, some of these lesions can be difficult to identify, and close evaluation of all branches is important. Imagine how limited we would be in trying to detect these small lesions without magnification. C. Photographic coning to area of lesion. Obstructing lesion and two adjacent filling defects (arrows) are evident in this patient. Preoperative ductography is done and then used to direct a wire localization of the lesion. |
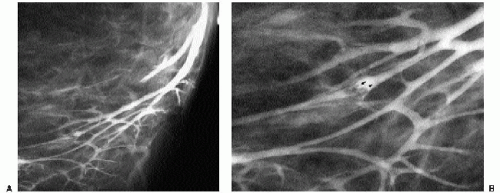 Figure 11.10 Papilloma, filling defect. A. Opacified duct is moderately dilated. Do you see the lesion? Despite the magnification technique, some of these lesions can be difficult to identify, and close evaluation of all branches is important. Imagine how limited we would be in trying to detect these lesions without magnification. B. Photographic coning to the area of the lesion demonstrates a filling defect (arrows) in the opacified duct. The edges of the lesion are irregular, consistent with contrast pooling in the interstices of the papilloma. Notice the distance from the nipple to the lesion. Although papillomas are often in a subareolar location, not all of them are. Without knowing the location of this lesion preoperatively, do you think the surgeon would extend the dissection to this point? Even if the dissection was extended to this point, can we be sure the pathologist would know where to look for the lesion for complete histological evaluation? |
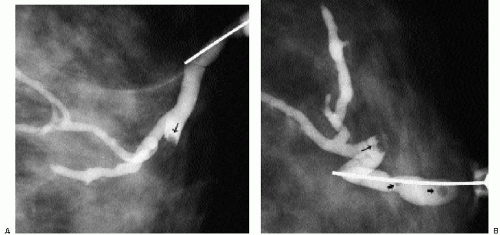 Figure 11.11 Papilloma obstructing side branch; air bubbles. Craniocaudal (A) and 90-degree lateral (B) views demonstrating a lesion (thin arrows) obstructing one of the branches of the opacified duct. The duct is dilated. Air bubbles (thick arrows) are well circumscribed and lucent. They are not seen on the craniocaudal view in this patient. |
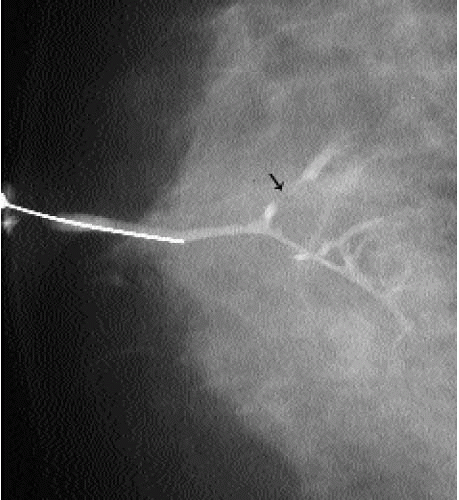 Figure 11.12 Papilloma, wall irregularity. Normal-caliber duct with apparent narrowing and irregularity involving a side branch of the duct (arrow). Ductographic findings for ductal carcinoma in situ and papillomas often overlap, hence the need to recommend biopsy. |
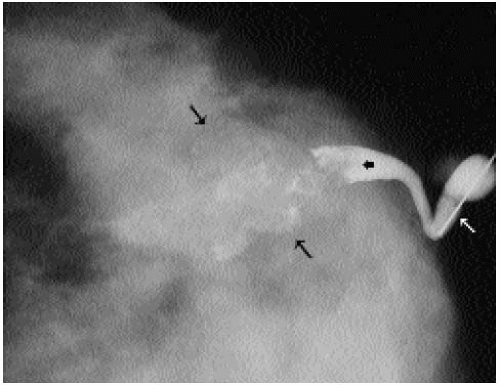 Figure 11.13 Papilloma, expanding and distorting the duct. This lesion (thick, black arrow) is obstructing the duct. Contrast (thick, black arrow) is seen seemingly outside the confines of the duct, but this is actually contrast in the interstices of the lesion, and the duct itself is normal. The duct is dilated compared with the cannula (white arrow). |
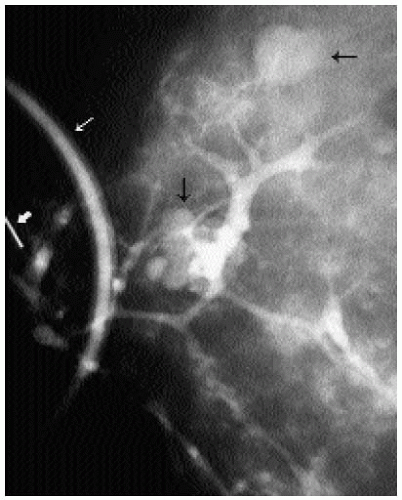 Figure 11.14 Fibrocystic changes, connection to cysts. Normal-caliber duct with contrast opacifying multiple cysts (black arrows). A portion of the contrast-containing tubing (thin, white arrow) used for the ductogram is seen superimposed on the breast. Ideally, the technologist moves the tubing away from the field of view. Portion of cannula (thick, white arrow) is seen. |
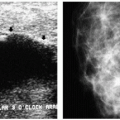
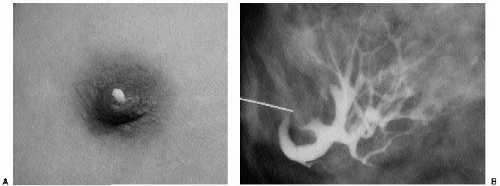 Figure 11.15 Duct ectasia. A. Thick, white discharge is seen commonly in women with duct ectasia. B. Different patient; dilated duct in its subareolar distribution. The more proximal branches assume a normal caliber. No focal finding is identified. |
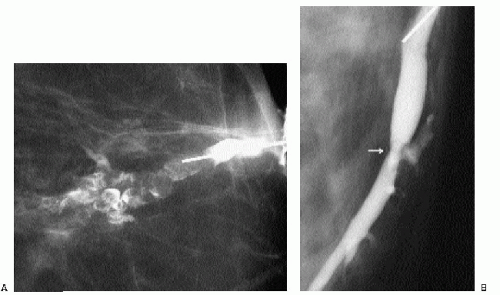 Figure 11.16 Ductal carcinoma in situ (DCIS). A. Intraductal lesion with interstices outlined by contrast. The duct is dilated between the lesion and the nipple. A papilloma with associated and adjacent DCIS (low to intermediate nuclear grade with no central necrosis) is diagnosed histologically. B. Different patient; focal area of narrowing (arrow) in opacified duct. The duct is minimally dilated. DCIS is diagnosed histologically. |
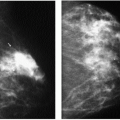
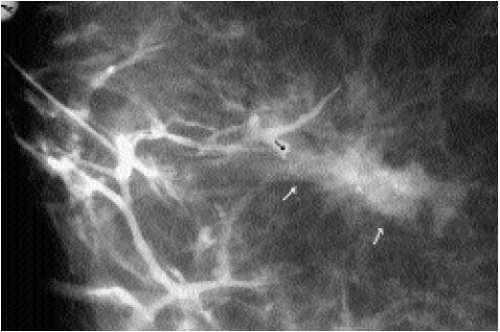 Figure 11.17 Invasive ductal carcinoma, not otherwise specified. Patient has a spiculated mass on her mammogram and spontaneous nipple discharge. The opacified duct is borderline dilated. A side branch of the duct is obstructed (black arrow), with a meniscus noted at the obstruction site. This corresponds to the area of the spiculated mass (white arrows) on orthogonal views (only one view is shown) consistent with an invasive ductal carcinoma presenting with nipple discharge and a mass seen on the mammogram. |
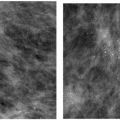
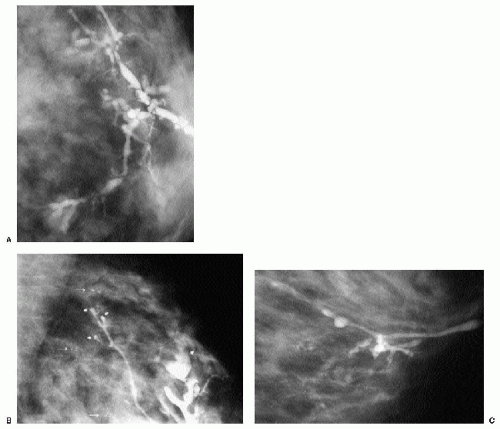 Figure 11.18 Ductal carcinoma in situ (DCIS). A. Craniocaudal magnified (1.8×) view of the anterior aspect of the left breast. Diffusely abnormal duct in a 42-year-old patient with spontaneous nipple discharge and a normal mammogram. This duct extends proximally in the upper central portion of the left breast. Multiple areas of narrowing and sacculation are identified, as are abrupt, rounded terminations of the duct. B. Mediolateral oblique magnified view posteriorly. Focal areas of sacculation are seen terminating several of the duct branches (thick arrows). Clusters of calcifications (thin arrows) are also noted on the magnification views, although not very striking on the routine views, however, with magnification, concern in increased. DCIS diffusely involving the opacified duct and surrounding tissue is diagnosed histologically. C. Different patient; diffusely abnormal duct with areas of sacculation and narrowing. |
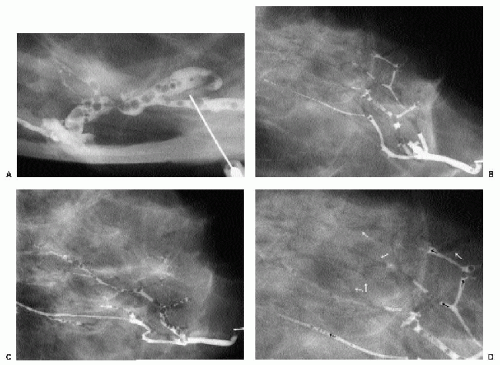 Figure 11.19 Air bubbles. A. Well-circumscribed, round, lucent filling defects. These change in position between views. B. Different patient. Craniocaudal (CC) and 90-degree lateral (C) views. Photographic cone down, CC projection (D). Air bubbles (black arrows) are present in the opacified duct, and there is air (white arrows) outlining proximal branches of the duct. The source of the air is not clear. Although there is dense tissue, the air is not apparent on the preductogram films, and yet no air was present in the syringe or cannula at the time of the injection. |
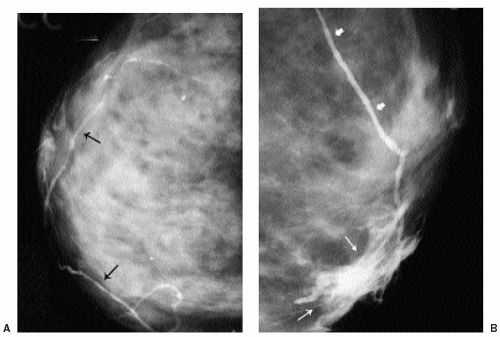 Figure 11.20 Opacified lymphatic channels. A. Contrast opacifies channels (black arrows) in a nonanatomic distribution for ducts. B. Different patient; proximal extravasation (thin arrows) resulting from an attempt to opacify the cannulated duct. Burning is described by the patient when the extravasation occurs. Contrast opacifies a channel (thick arrows) in a nonanatomic distribution for a duct. Opacification of lymphatics is seen in some patients with proximal contrast extravasation, as in this patient. |
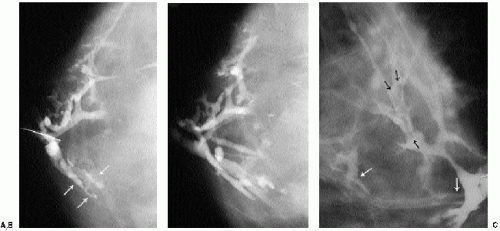 Figure 11.21 Pseudolesions. A. Diagnostic ductogram demonstrates a diffusely irregular duct with filling defects and wall irregularities (white arrows). Excision is recommended. B. Preoperative ductogram demonstrates a normal duct. Previously noted abnormalities are not reproduced. Nonspecific fibrocystic changes are reported histologically. C. Different patient; tubular-like filling defects are noted in different portions of this duct (arrows demonstrate extent of filling defects). It is unclear whether these represent duct contents. |
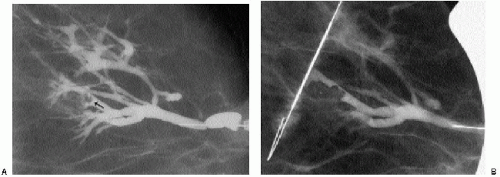 Figure 11.22 Papilloma. A. Diagnostic ductogram demonstrating a filling defect (arrow) in a side branch of an arborized duct. B. On the day of surgery, the ductogram is repeated and used to guide a wire localization. Midportion of reinforced wire segment is just posterior to the intraductal lesion. |
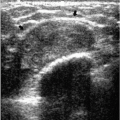
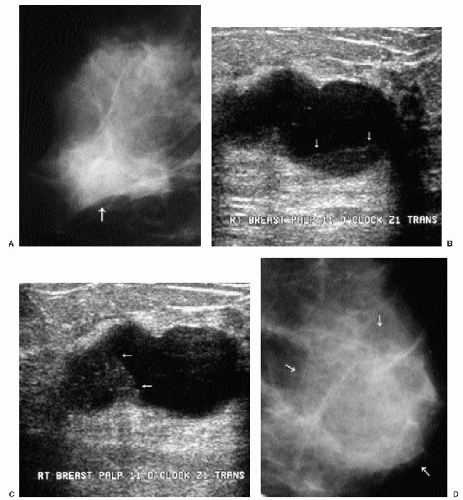 Figure 11.23 Cysts. A. Right mediolateral oblique view. A mass with obscured margins (arrow) is imaged corresponding to a palpable area. B. With the patient in a supine position, ultrasound demonstrates a macrolobulated mass with posterior acoustic enhancement and internal echoes (arrows) in the dependent portion of the cyst. C. Decubitus position. Internal echoes have now shifted into what is now the dependant portion of the cyst (arrows). This shift in the echoes confirms that the finding is a cyst. When we can establish the diagnosis of a cyst, we do not routinely undertake aspiration unless the patient is symptomatic or requests it. D. Different patient. A mass with obscured margins (arrows) is imaged corresponding to a tender lump. E. A cystic lesion with posterior acoustic enhancement is imaged corresponding to the area of concern to the patient. Internal echoes and apparent septations are noted (arrows). The wall is not sharply defined. Aspiration and pneumocystography are undertaken for diagnostic purposes. F. Needle with tip in the center of the cyst. The aspiration is monitored with real time ultrasound, and many of the echoes are seen being aspirated into the needle. The wall of the cyst is not sharp. This is often seen with tender, possibly “aseptically inflamed,” cysts. After the contents are aspirated, 50% of the volume of fluid aspirated is replaced with air. Craniocaudal (G) and 90-degree lateral (H) double spot compression magnification (1.8×) views following the injection of air. A smooth-walled cyst cavity is seen with no intracystic component. There is wall thickening, and the surrounding tissue is normal. |
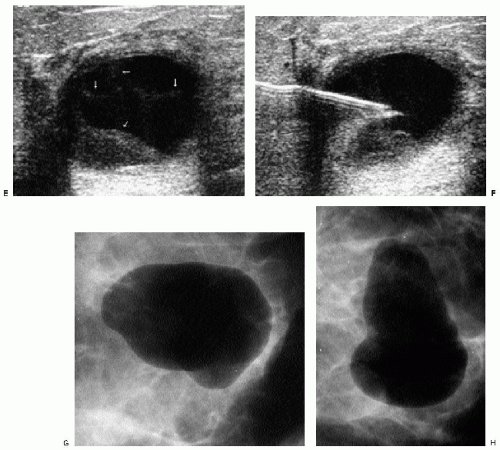 Figure 11.23 (continued) |
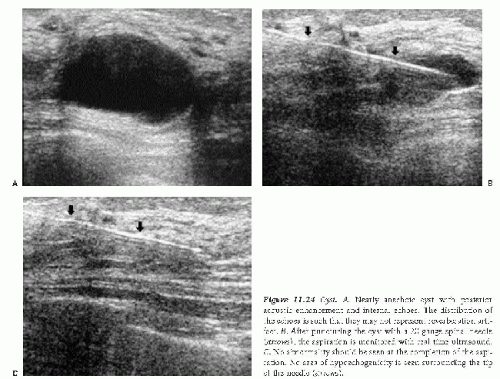 Figure 11.24 Cyst. A. Nearly anechoic cyst with posterior acoustic enhancement and internal echoes. The distribution of the echoes is such that they may not represent reverberation artifact. B. After puncturing the cyst with a 20-gauge spinal needle (arrows), the aspiration is monitored with real time ultrasound. C. No abnormality should be seen at the completion of the aspiration. No area of hypoechogenicity is seen surrounding the tip of the needle (arrows). |
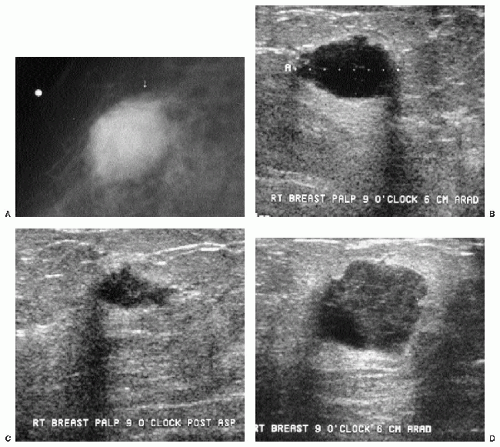 Figure 11.25 Poorly differentiated invasive ductal carcinoma, not otherwise specified. A. Spot tangential view in a 36-year-old patient who presents with a tender lump. A round mass with microlobulated and ill-defined margins is seen. B. Complex cystic mass with internal echoes and posterior acoustic enhancement. Closely evaluate the margins and note irregular microlobulations. Aspiration is undertaken. C. Residual irregular abnormality is seen after aspiration. The fluid is submitted for cytology. Necrosis, inflammatory cells, and viable cells with atypia are reported. A trial of antibiotics is recommended with a follow-up ultrasound in 4 weeks. D. Five weeks later, a round mass with a heterogeneous echotexture and posterior acoustic enhancement is imaged at the prior aspiration site. Ultrasound-guided core biopsy is done to establish the diagnosis. |
evaluate the wall of the cyst and the appearance of the surrounding tissue (Figures 11.26 and 11.27).
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


