Jugular/clival paraganglioma – delayed postembolization, multisession radiosurgery for growing residual
SKULL BASE REGION
Petroclival/jugular foramen
HISTOPATHOLOGY
Paraganglioma
PRIOR SURGICAL RESECTION
Embolization
PERTINENT LABORATORY FINDINGS
N/A
Case description
This 44-year-old woman was investigated for left hypoacusis, tinnitus, and left hemitongue hypoesthesia and hypomobility. Imaging was compatible with paraganglioma of the jugular foramen, with infiltration of the occipital condyle and lateral portion of the clivus. An embolization procedure was performed prior to the planned surgery. However, surgery was canceled due to the development of significant new deficits such as dysphonia, swallowing difficulties, and left facial weakness (House-Brackman [HB] grade 2). Radiological follow-up showed a reduction in the volume of the lesion due to internal necrotic cystic degeneration, which was associated with partial resolution of symptoms. At 3-year follow-up, brain magnetic resonance imaging (MRI) revealed tumor progression ( Figure 10.53.1 ). Multisession stereotactic radiosurgery (SRS) (25 Gy in 5 fractions at the isodose of 82%) was performed using CyberKnife ( Figure 10.53.2 ). Follow-up imaging at 5 years showed a volumetric reduction of the lesion. From a neurological point of view, improved left facial deficit (HB1) and stabilization of other cranial deficits were also observed.
Radiosurgery Machine
CyberKnife
Radiosurgery Dose (Gy)
25, at the 82% isodose line
Number of Fractions
5
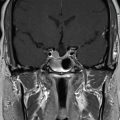
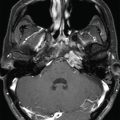
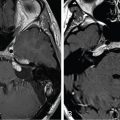
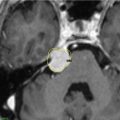
Figure 10.53.1.
Postcontrast T1-weighted images prior to stereotactic radiosurgery.
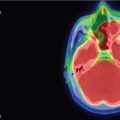
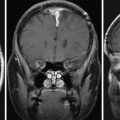
Figure 10.53.2.
Imaging of the treatment plan.
Critical Structure
Dose Tolerance
Brainstem
14 Gy maximal in single session stereotactic radiosurgery (SRS)
<1cc >10 Gy
Not established in multifraction SRS
Lower cranial nerves
25–30 Gy in multifraction SRS
Only gold members can continue reading. Log In or Register to continue
Apr 6, 2024 | Posted by drzezo in GENERAL RADIOLOGY | Comments Off on Jugular/clival paraganglioma – delayed postembolization, multisession radiosurgery for growing residual


 Esthesioneuroblastoma – delayed postoperative radiosurgery for recurrence at long-term
Esthesioneuroblastoma – delayed postoperative radiosurgery for recurrence at long-term
 Null cell – delayed postoperative radiosurgery for growing perioptic residual
Null cell – delayed postoperative radiosurgery for growing perioptic residual
 Chondrosarcoma – definitive radiosurgery after subtotal resections
Chondrosarcoma – definitive radiosurgery after subtotal resections
 Large vestibular schwannoma – delayed postoperative radiosurgery for growing residual
Large vestibular schwannoma – delayed postoperative radiosurgery for growing residual
 Trigeminal neuralgia due to petroclival meningioma – upfront radiosurgery
Trigeminal neuralgia due to petroclival meningioma – upfront radiosurgery
 Superior sagittal sinus meningioma – delayed postoperative, multisession radiosurgery for growing residual
Superior sagittal sinus meningioma – delayed postoperative, multisession radiosurgery for growing residual



